It's been a terrible season for respiratory infections (RSV, Covid, Flu) and gastro bugs, the most vulnerable can't afford to eat, let alone turn on the heating, and social care availability has been in decline for a decade, worsening significantly in the past year, nuking front-door availability at hospitals, doctors and the transport they rely on.
All of which I mean to say: No. Shit. Sherlock.
It's all so painfully obvious to anyone paying attention. The doctors and nurses and care homes and mental health workers have all been screaming about this for a decade. Cuts upon cuts upon redirected funding upon private providers upon universal credit cutting benefits upon cuts and failures and all that before covid, all before inflation lowering everyone's incomes.
We need to hire. We need to train. We need to retain. We need to build. We need to instill the fact that care home workers, pastoral carers for our elderly are such bloody important roles because without them helping people live outside hospital, nobody else gets seen. We need to pay them, we need to pay them to pick up shit and talked to dementia sufferers more than Jeff Bezos can pay them to pack boxes.
If we can't do that… It's over. But we need to have a serious conversation about what we actually want to do with the infirm in this country. Letting them freeze to death in their own homes feels like state-mandated euthanasia without the "eu". Huh, a wild Brexit joke appeared.
1. Find some convoluted way that it's actually the fault of people who need treatment or front line staff and hammer that in compliant media and have it regurgitated by the BBC and pundits till it becomes received wisdom
2. Some sort of window dressing policy/mandated clapping and declare mission success. Anyone who continues to criticise about the fundamental problems is shouted down as just being anti-tory/political activist. E.g the other days wheeze where we banned plastic cutlery therefore releasing tons of human waste into rivers on the regular doesn't matter anymore.
The bit I'm curious about is if that is done deliberately or if British people are just culturally favourable to flagrant gaslighting.
No disagreements on your points. But I think we're a small country with a few very pervasive news outlets —mostly controlled by right-leaning billionaires— and a few far-right commentators who get disproportionate focus through outrage. I don't think we're special.
It's the same trap that a lot of countries fall into.
The NHS has also been deliberately weakened by the Tory (and Labour) to justify its privatization. That is the crucial point. The unusual seasons would just be a small extra burden if they had not weakened it.
This is such an unhelpful take. The UK government did Brexit while, for example, promising to redirect all the funding that went to the EU towards health care. Did it go to health care? No. Did the money go to Ukrainians? No. The government simply doesn't care about its populace, regardless of what's happening in Ukraine.
> The UK government did Brexit while, for example, promising to redirect all the funding that went to the EU towards health care. Did it go to health care? No.
That reads like you resent Ukrainians for getting support.
I'll charitably read it as "they only care about the optics" because these governments didn't need a war on their doorstep to cut funding to councils for social care, let public pay rot under inflation, pay their mates through preferred tender, repeatedly push front line workers to the brink, cut the nursing bursary, push out senior doctors by ubertaxing their pension contributions, kick medical infrastructure projects down the road again and again and again. Remember Boris built 40 hospitals with his bare hands.
It's great if we've been able to help Ukraine. But it's immaterial to health and social care in this country.
How is that? How do you suppose the British government could have avoided this? You speak of Ukrainian lives, so presumably you are referring to foreign policy and not domestic policy. Through which foreign policy decisions has the British government caused this?
It's not like Britain could have kept energy prices down by not aiding Ukraine. It's also hardly realistic to suggest that British aid to Ukraine has come at a significant expense to the taxpayer, given the baseline defence spending by Britain to counter Russia.
Could covid be the last straw to the NHS that A&E can't serve patients in a timely manner?
I have experience the 48 minutes ambulance wait second hand. A friend of mine was having heartache and called ambulance. He was told to wait for 45 minutes. His wife insisted to drive him straight to A&E instead. The moment he steps out of his car he crashed. That's was about 20 minutes after the emergency call. Had he waited longer he would be gone.
On another occasion, I had simultaneously received a letter from NHS, telling me to return for minor operation, and a phone call from doctor, telling me no further follow up needed. I can't reach the doctor through phone call so I go for the consultation anyway. Turns out the hospital did schedule an appointment for me, a different doctor did prepare to perform a biopsy on me, upon further clarification, the doctors did discharge me. I wonder how much is it due to the system being overwhelmed, how much is just normal error.
A personal anecdote: had been feeling very unwell all morning with back pain but needed some fresh air so went for a walk, on the way back my chest tightened to the point where it felt like a very heavy person was sitting on my chest and was having stabbing pains. I'd never experienced anything like this before.
My local GP was near by so I went there first, described what was happening to the receptionist... they said 'Call 111' (NHS non-emergency triage, for non-Brits) and shoo'd me off; I loitered around and Googled symptoms and yea... 'possible heart attack, go to A&E NOW' was the general gist. Called 111 from within view of the receptionist in case I collapsed, 15 minutes later I'm still on hold - I figured all they'd do would put me through to 999 after spending 10 mins asking questions.
Got an Uber to A&E, and had an EKG within about 20 minutes of arriving. They said it's not a heart attack, probably isn't myocarditis or pericarditis, then the weird question 'do you suffer from anxiety or any mental health problems?'...
I'm 100% sure it wasn't psychosomatic or an anxiety attack. But that was the point where their concern ended and I was discharged with no follow up from GP or any idea of what had happened. Turns out, it was acute pancreatitis caused by a gall stone - I had to pay privately to find that out because repeated GP appointments they couldn't care less.
Either way, it's an absolute clusterfuck, and this same pattern of systemic dysfunction has been repeated with pretty much every interaction I've had with NHS funded services (both hospitals and GPs), and I'm fairly sure - like in a_c's friends case - if it had've been a heart attack it would've required me to drop dead in the GPs reception for them to do anything more than just pass the buck.
The UK is down with leading countries like Colombia in the doctors-per-capita rankings. The NHS could be a lot better, and most doctors want it to be a lot better. If there aren't enough doctors to provide an adequate service - and there really aren't - it's not the front line staff who are to blame.
Is it not the same doctors that vote to cap the amount of doctors places in higher education in order to protect wages? Why are we not training as many doctors who meet the educational requirements as possible? Every year come A Level results there’s a kid in the paper with AAA grades who can’t get into medical school. It’s a disgrace.
> Despite the NHS’s clear need for more medics, the number of medical and dentistry students each year is capped by the government to control costs, as it subsidises the courses.
> The Secretary of State for Education, James Cleverly, commented recently that it's not possible to "flick a switch" to increase the numbers of doctors undergoing training, due to having to ensure there is enough funding and capacity for teaching and placements.
I did not know this thank you for bringing it to my attention. Seems like a pretty feeble excuse from Cleverly though. In my opinion, anyone who's capable of it and wants to should study Medicine should be supported in doing so because the societal benefits are so great. The fact that we stop 17,000 from doing so is an absolute disgrace. We waste money on a lot of shit in this country, I'm sure the money could be found to send more people on to study medicine. It seems to be universal across the country that councils lay new block paving only to dig it up a few months later on a whim for some reason or another, that could be a place to start.
Depends on how you see it, medical degree is a supply chain problem, subjected to the same bullwhip effect. We can't predict demand of doctors 5 year down the road. The worst we could do is to treat today's demand as demand for 5 year in the future. If we double the supply today, in 5 years we will have double supply, hopefully without another pandemic. Many things could happen, if funding stays the same, benefits among all doctors will be affected, or we appropriate funding from other endeavours. If the demand doesn't sustain, funding get cut, less students find it attractive as a career, supply reduces. In reality many more factors get into play. So when Cleverly said "we can't flip a switch", there are some merits to it.
Oddly enough, I’ve heard the same thing regarding doctors voting for a cap. Wonder where that’s from?
It’s an awful excuse; I agree with you. If we were to be quite "cold" about this and think of it in a purely beneficial sense to the economy, surely the economic benefits of a healthy population far outweigh the costs, although I imagine it’s quite hard to "quantify" such a measurement?
That's an interesting idea, but a lot of people in the profession would reject a move like that, as it would put downward pressure on their earnings (amongst other things):
> BMA meeting: Doctors vote to limit number of medical students (Andrew Cole)
> Delegates at the annual BMA conference voted by a narrow majority to restrict the number of places at medical schools to avoid “overproduction of doctors with limited career
opportunities.” They also agreed on a complete ban on opening new medical schools.
> David Sochart, from Manchester and Salford, warned that in the current job climate allowing too many new doctors into the market would risk devaluing the profession and make newly
qualified doctors prey to “unscrupulous profiteers.” A glut of doctors would undermine competition and would therefore lower standards and ensure mediocrity, he claimed.
He said, “Patients and health care should not be treated as mere commodities, and neither should medical students. We must not allow another lost tribe of doctors to be consigned to the wilderness.”
> Grant Ingrams, representing GPs, said that doctors should not be trained if there was no job at the end. He warned that this could spark another “brain drain,” adding: “It is wrong and immoral and a waste of taxpayers’ and students’ money.”
> But Paul Flynn from the consultants committee said that the root problem was a lack of effective workforce planning and warned members against a kneejerk response. “This is what
blighted workforce planning. It would be hypocritical if we were to do it ourselves.”
> The BMA’s chairman, Hamish Meldrum, said he sympathised with the sentiments of the motion but asked members to vote on evidence rather than “gut reactions.”
“We want to see an expansion of [the numbers of] GPs and consultants,” he said, “and for that we need more students.” But the motion was passed by a small majority (58% versus 42%).
> Members also agreed to a motion accepting that some specialties might need to raise the total number of years spent in training to accommodate the demands of the European Working Time Directive.
> Stephen Austin, from the consultants committee, said that the time needed to acquire the necessary competences was likely to increase—especially in procedure based specialties—and that the only sensible solution was to increase the total amount of time in training.
> Members also voted to press for an agreed minimum national level of funding for study leave to overcome the widespread national variation in the amounts that are currently available.
It's honestly an absolute disgrace. Train them, and if there are no jobs, let them go overseas and work. The government constantly bangs on about Britain's 'reputation overseas' what on earth could do more good for it then literally exporting people who save lives. I honestly can't see any justification for this other than doctors profiteering and it makes me sick to my stomach.
The British Medical Association is in a position to veto changes to the number of medical students being educated in the UK, as its members have a monopoly on providing medical training, which is why they hold votes on such things at their conferences:
Matters like this are normally discussed behind closed doors, and there is plenty of horse-trading, with favours being negotiated, and assurances, and understandings that are reached before major changes are "unilaterally" "announced" by the Government. There are different factions within the medical profession, and none of them want to lose out when there are changes. Priced into the government's announcement they they are going to train more doctors, therefore, are a range of promises and commitments to the medical profession to make sure that this will proceed without incident.
Interesting, thanks for that. Do you know if that only happened the once? I can’t find references to another vote like it.
From what I can see elsewhere, the tone seems to have changed slightly since then?
> “We welcome the news that there will be extra funding for medical school places as this desperate need for more doctors in training is a recommendation that we made in our Medical Staffing in England report, which we issued last month.“
> “However, this increase in student places must not come at the expense of extra funding for the existing workforce or reductions in funding in future years, because tackling the waiting lists and backlog are going to require sustained investment over many years. And the government must make clear that there will be sufficient clinical placements for all those who succeed at medical school.
A generous take on it seems that the BMA don’t want to make things worse for existing doctors.
I suppose if the government funded the NHS more, ensured that existing doctors wouldn’t be worse off, one would hope that the BMA would be fully supportive of training new doctors?
I suspect that this was one of the first years that reports from that conference were made available in a digital format, and that the way that issues like this have been dealt with subsequently has taken into account the likely impact of similar documents coming to wider public attention. I don't think it's something that people have stopped talking about in their professional circles, and I imagine senior figures would be able to tell ministers exactly what people think and what would happen.
Part of the difference is probably that the 2021 article is a press release aimed at the public, rather than an internal discussion that lead to a vote. With enough money I imagine you could make everyone happy, and doctors' standard of living is at just as much risk of being inflated away as anyone else's, so it's no surprise that the professional body would support training more doctors subject to guaranteed funding including for medical educators and clinical placements (all of which will have a direct impact on their members' salaries, bonuses and allowances). How exactly that will work out, and how's it's going to play to the public, we'll have to wait and see.
> In short, the NHS is more correctly seen as nationalised rather than socialised medicine, achieving the first three levels of a socialist health service identified here. It can be said to have socialist principles in the limited distributional sense and has some socialist means to achieve these.
The study is from 1997, and the NHS has definitely changed in the 25 years since, arguably becoming more privatised since the Health and Social Care Act 2012 (among other decisions).
The UK generally does somehow manage to hit the sweet spot of all the expense and duplicated effort of market solutions with all the remote decision making and political weaponisation of government solutions and get the worst aspects of them both.
Now imagine you'd had to pay thousands of dollars for that trip to the ED. Otherwise that doesn't sound any different from an experience with the medical system in the US. One of the first questions you're asked is if you have insurance (in Texas it's not assumed), so they can determine what class of patient you are.
My 2 penny opinion on this debate is people should always refer to the UK government rather than the "NHS". The NHS is just a government department run by the health minister. Saying the NHS is in trouble means you're not pointing your finger at the people responsible. (Your opinion on this is very welcome)
Are you talking about how NHS Scotland is run by the Cabinet Secretary for Health and Wellbeing based out of Holyrood? Please tell me you're not. It's not really very relevant to the discussion.
My point was that it's the government running the health service. Name and shame the person responsible.
The funding is given to them by the uk gov. They are allowed to elect how they spend it. If the funding is insufficient then it’s not really fixing the problem.
Covid has exacerbated the issues caused by the Conservative government's 12 year underinvestment in the NHS. They have spent about 30 billion less than is needed, according to the figures I've seen. Example:
They need to spin out how the NHS funds itself into an independent body like the BBC Trust (BBC Board these days). The NHS should be able to set a budget and levy taxes accordingly in order to meet some key targets it sets itself. The union should be part of this too.
These taxes should show up as a health levy on people's paycheques like they do in British Columbia.
This body should be responsible for education, recruiting and staffing be it via universities or immigration.
This is a great idea, so long as the same body has the power to decide how the NHS is structured and managed too, free from central government interference. Accountability seems totally absent anyway, so let them just get on with it.
The Conservative government are deliberately running it into the ground and only true independence in terms of funding and management would be enough to isolate it from further sabotage.
> This is a great idea, so long as the same body has the power to decide how the NHS is structured and managed too, free from central government interference.
That's the idea. Not sure how the the board would be chosen mind, elections along the lines of PFCC? If ministers were involved it would probably devolve into the status-quo.
It’s not really Covid or shifts in behavior, it’s a policy decision by political Tory leadership of how much margin in the system of the NHS to maintain. And imho in their case their policy is negative margin in order to increase privatization of healthcare in the UK.
It'll still probably take a few more years to get the full picture of what the cost of the lockdowns was since it takes so long for the statistics to be collated.
For example, turns out the lockdowns got one of my family members by making it difficult to get a diagnosis on what turned out to be a cancer. Hopefully the 6 months (approx) delay on getting it dealt with doesn't turn out to be important.
I wish the best as well. But don't forget that at the same times all kind of other people had to move or cancel their treatment because the hospitals were full. What weighs heavier is for the statisticians to figure out.
The graph you linked shows that Sweden has ~70k deaths in 2022 up until September 30th, thus you'd have to add about a third (for Q4) which would result in 93k which would mean it's a little higher before the years before the pandemic. Anyway, one would have to wait to see the stats of Q4 to really talk about it (I think usually Q4's are higher than other quartals because of winter). As such, your point is moot.
We've had 3 years of reduced exercise, and people are 'making up' for being cooped up by engaging in more activities that they couldn't before. Taking those road trips, going to that amusement parks, snowboarding, mountain biking, etc.
Not to mention supply chain shortages in medical and medical-adjacent fields, paramedics, etc. at a time where some people have overlooked long COVID symptoms
As well as an economic depression at a time where we're suffering a cultural PTSD from the previous few years.
Even if COVID isn't found directly responsible for these deaths, I suspect it is indirectly responsible.
Mental health down the drain too. I know this will be an unpopular HN opinion but WFH has made me feel socially isolated. I can’t stand working alone all day anymore and I’ll be looking out for a job that has a real office where most people come in this year.
I don't think it'll be an unpopular opinion that WFH isolates you. I've worked from home for two decades and you spend a lot more time on your own and you have to do something about that. I think many people like working with other people some of the time.
What may be unpopular is the idea that you need a workplace that enforces on-site working for remote-possible work being a requirement to get your daily social interactions done. You're essentially saying you're looking for an employer that cares more about their middle management than their workers. Just be careful what you wish for.
The problem I have is that because I didn’t get social interactions at work anymore, I have to get them outside of work time. I can’t just enjoy a game alone anymore because I’ll end up having socialised with no one and feel depressed.
So I’m left either deciding if social interaction or personal time is more important. While previously when working in the office I got both.
Going out a few days a week really just doesn't replace the same fulfillment as spending most of the day 5 days a week working with others. It's so easy to go a day without talking to a single person when working from home which is just depressing. I have such great memories of past jobs, things like putting out a big release or making a big sale and everyone going out to the bar to celebrate, lots of coworkers I still communicate to regularly. Friday night drinks, board games and stuff in the office.
The current job has just been sitting at home endlessly.
It may be relevant and of interest to readers around the world to learn how we in Britain access the NHS, our envy-of-the-world National Health Service.
The main way is via your allocated General Practitioner (GP). To see a GP you need to telephone the GP's place of work, known as a surgery, and to have any chance of getting a same day appointment you need to call at 8am precisely. Don't call at 7.59 because you won't be connected, and don't leave it until 8.01 because it will be far too late. Call within the first few seconds after 8am and you'll be informed that you're in a queue, behind several dozen earlier callers.
After an hour of waiting you'll get through to a non-medical receptionist who will ask you about your symptoms, and make a judgement about whether or not you or your child is worthy of one of the few remaining appointments for that day. If you're a very pushy mother, or someone who really enjoys talking with GPs' receptionists (which most people don't) then you may have some success in this. If you're just a chilled out guy who doesn't like to fuss, you've got no chance.
You'll then be informed that to make an appointment for a later date you need to try again for a same-day appointment the next day by repeating the process above the following morning. It is not possible to arrange an appointment for any time further in the future no matter how long you are prepared to wait.
The only other means of accessing the NHS is by rocking up at the Accident and Emergency (A&E) department of your nearest large enough hospital. Unsurprisingly given the above, these are rather busy and you may be waiting for a day or so before you get seen. To avoid adding to this delay you should make you own way to A&E because ambulances routinely take several hours to reach you for the most urgent cases (heart attacks, stokes etc) or up to a few days for, say, a fallen elderly person, and on reaching the hospital you wont be able to leave the ambulance and enter the A&E department for up to another day.
However, once you're in the system and being seen by a specialist then by all accounts you do get fairly well looked after, so putting in the hours at A&E or regularly playing the GP telephone lottery may well prove worth your while if you wish to make use of our envy of the world NHS.
For what it's worth this is quite similar to my experience here in Sweden except:
- you speak to a nurse on the phone, not a non-medical receptionist (frankly, that sounds insane)
- the Vårdcentral (equivalent to surgery) prioritizes children in my experience
- your Vårdcentral is not allocated, but you can choose one. Some have better capacity, some have worse.
- there is another layer between Vårdcentral and Akuten in a hospital called Närakuten where you can go to get checked out. The waiting times are anywhere between 30 minutes and a couple of hours.
I would even guess that the British situation is not unique but the medical system is overloaded everywhere in Europe.. Most people I know, including myself pay for private care.
> The main way is via your allocated General Practitioner (GP). To see a GP you need to telephone the GP's place of work, known as a surgery, and to have any chance of getting a same day appointment you need to call at 8am precisely. Don't call at 7.59 because you won't be connected, and don't leave it until 8.01 because it will be far too late. Call within the first few seconds after 8am and you'll be informed that you're in a queue, behind several dozen earlier callers.
1) Genuinely baffling to see people who think their individual sucky experience is universal. What you describe is how your gp works. Change GPs! There are better surgeries around.
I called my GP after 12 midday and explained that I had turned a bit yellow and had pain under my right ribcage, and they booked me in for an appointment a couple of hours later, and after I'd send them they booked me into my local hospital's surgical assessment unit (thus bypassing A&E) where I was hooked up to IV fluids and antibiotics. I got scans that day, I got surgery the day after, I was discharged a few days later when the infection had clear and my numbers were better.
Same day appointments are for emergencies, and if you have an emergency you will get a same day appoint
> The only other means of accessing the NHS is by rocking up at the Accident and Emergency (A&E)
No, this simply isn't true. In this order depending on severity of illness, people can chose to get support from: NHS Website, NHS 111, Pharmacy, GP, Minor Injury and Illness Units, Emergency Departments, or Ambos.
Plenty of services now have self referral - podiatry, physiotherapy, dietetics, eating disorder, mental health crisis, antenatal, etc etc. So you don't have to go via your gp, you just phone them up and make an appointment.
I think you may be suffering from some quite literal survivor bias.
Okay, I may have over-extrapolated for effect, after all some surgeries don't even have telephone queuing, you just keep getting the engaged tone and redialing until your call is finally answered at half past ten, to be told the same thing.
I don't know the exact circumstances of your case but it sounds quite likely you wouldn't have lived to tell the tale if you'd been registered with my GP.
I think you're overestimating the ease with which most people can swap surgeries, and you're definately overstating the extent to which your list of NHS hacks are a realistic prospect for most people, who by and large don't even want to bother thier doctor unless they really have to, and then when they really have to - they can't.
I think this is a common framing because not everyone is aware that GPs are independent private businesses. We always refer to them as "part of the NHS" as if they were (or at least should be) equivalent to each other.
You missed one important entry point: 111 can refer you to an Urgent Care Unit. There are growing numbers of these in town centres and hospitals. It's basically an extra GP resource.
"The difference in 2022 - compared with 2020 and 2021 - is that Covid deaths were one of several factors, rather than the main explanation for this excess"
One of the other factors is the crisis in the NHS:
"At the start of 2022, death rates were looking like they'd returned to pre-pandemic levels. It wasn't until June that excess deaths really started to rise - just as the number of people waiting for hours on trolleys in English hospitals hit levels normally seen in winter."
So, I don't think people's propensity to go into lockdown is particularly relevant here.
I didnt want to imply to go into lockdown, i was more pointing at the lack of interest in the current non covid excess mortality. This data has been out there for a while and not just in the UK. Could have worded it better.
I read a paper in 2016 that was attempting to understand if there was a human cost to Austerity.
They succeeded in finding a causal link between austerity measures and increased mortality.
At the end of the paper they estimated that 120,000+ people have died as a result. Additionally: that the the rate of excess deaths was increasing year on year.
There is an issue with highlighting this;
For starters, many people are very likely to bury their heads in the sand:
* "How do you know that it's related to Austerity" (not reading the paper)
* "They would have died anyway"
* "The world is different from the time period it is modelled from" (it corrects for this by comparing also to other roughly equivalent economies)
* "The UK is different than other advanced economies!"
The other issue is that it sounds so insane and conspiratorial.
120,000 is a large number. It's approximately the size of Stratford upon Avon.
A follow up study puts the number now closer to 330,000, around the population of Coventry.
Somehow people will blame the NHS for not being efficient, though evidence to the contrary exists throughout its history, often being one of the most cost effective healthcare systems in operation; or that COVID is a contributing cause to these figures.
People are unwilling to hear this: This was a problem well before the pandemic.
Both underfunding and overfunding can cause inefficiencies, there is a sweet spot in the middle where an organisation would be at its most efficient.
It's quite clear that the NHS has been underfunded, and under resourced, for the last decade. However the government still try to argue that the inefficiencies are a organisational problem rather than a funding problem. Which is still laughable when they have presided over it during the whole time period in question.
And to be clear if you have an overfunded health system then you are providing good medical treatment to your population in a timely manner. You're just spending more money doing it than you might otherwise do so.
So someone with ethics might argue that if you are in an uncertain area between over and underfunding then it will kill fewer people to err on overfunding.
Which is exactly how the semi-privatised NHS operates. Agencies have been encouraged to set up as independent service providers who can profiteer by price gouging the NHS while paying nurses and doctors pocket money.
Renationalising the NHS and limiting the private sector to those few expensive services that are essential would fix this.
But both political parties are working for the people who profit from this situation.
They would be better off addressing the root causes that are sending more and more people to the NHS in the first place. Healthy food needs to be cheaper than unhealthy food, physical exercise needs to be encouraged at a grass roots level, working conditions need a massive overhaul, education needs to improve, salaries need to rise and/or rents need to fall, and housing needs to be of better quality, particularly around insulation. At the minute we’re treating the symptoms and not the cause of the disease.
Not necessarily: my understanding is that in the US a few people probably get more healthcare than the optimum, and many get less, all on an extremely large budget.
What does overfunded even mean for a health system? Some patients with serious complex conditions can consume an effectively infinite amount of healthcare services, especially if we want to take heroic measures to keep them alive a bit longer. I don't think there is any amount of funding that could realistically be put in that would make the UK NHS overfunded; you can only compare funding and outcomes relative to other developed countries.
The "funding" problem that I never see discussed is that the NHS costs massively more per-person now than when it was introduced.
ex. How many ambulances at a few pounds in 1948, which were vans with a stretcher in the back and a couple of blokes to drive it. What about 2022? The cost, roughly £150K for the ambulance, goodness knows what to train up ambulance technicians and paramedics. If the kit is broken, the ambulance can be out of service, which means more units to provide cover (or not if you can't afford it!). The on top of all that, many more people go to hospital because the care is leagues above what you got in 1948.
Ditto for equipment costs like Digital XRays, MRIS etc.
All of that is not surprising or even undesirable but it would be interesting to see the additional tax that you should be taking per-person to pay for all of this additional equipment. If the NHS costs around 30% of expenditure i.e. 30% of my tax then roughly 7.5% of my income covers the cost of the NHS, maybe £6K per year. When we look at things that way, you can see why the Government doesn't want to take any money in tax because that sounds like a lot of money. You can also see how they can't reduce costs by going backwards in replacing high-tech with no-tech.
It wouldn't need any more tax. There's a black hole in the budget caused by inefficient tax collection, almost entirely to the benefit of large corporations and very high net worth individuals.
There are also some quite ridiculous cash handouts for little or no taxpayer benefit. Like the notorious £37bn that failed to provide an efficient Covid test and trace system. Or the >£100m in the Michelle Mone scandal, which seems to have been just one of many. Or the £45bn in tax cuts in Kwasi Kwarteng's recent budget, which were supposed to "promote growth" but have done the opposite.
The UK is one of the richest countries in the world. It has also become one of the most corrupt.
i don’t think you realise how much the health service costs. you can tax all of the richest and it will represent a few days of the health budget. a new funding model is needed. otherwise there will have to be tax increases.
The NHS also costs more now because the population is sicker than in 1948. Older, fatter, more sedentary, heavily impacted by preventable chronic diseases. Demand for services is way up. Higher taxes might help a little but won't address the root cause.
From what I read it’s not the equipment, but a bloated layer of bureaucratic management on massive salaries that is the real issue. The front line staff get pittance in comparison.
> It is extremely difficult to find an accurate figure for the number of managers in the NHS, and most sources of information use different definitions for who is counted as a manager.
I’m not sure I can take the report seriously after that. You can’t write a report on management in the NHS and refuse to give a definition of manager. Also, how many of these managers are directly employed by the NHS and how many are employed as consultants?
I’m not saying you’re necessarily wrong but that report is hand wavey.
The Kings Fund is a credible source of information about the NHS systems in England, Scotland, Wales, and NI. One of the reasons that they're credible is because they're cautious about definitions. In your quote they're saying "lots of people have written about this, and they all use slightly different definitions for management, and so they all give different numbers".
What is a manager? Are you only including non-clinical staff? Or do clinical staff count too? If you're including clinical staff, how many hours of their working week are you counting as clinical hours and how many are you counting as managerial hours? Are you converting people who work part time as managers to Full Time Equivalent positions, or not?
I think that's the problem with "what I read". I think the "man on the street" would probably agree but not necessarily from hard data, just from the fact it is easy to blame inefficiency rather than structural or human problems.
"The NHS is full of bureaucracy" but it is a bureaucratic system so of course it is. People to charge hospital costs back to GPs, people to investigate trends and make sure that some GPs are not under-referring people to hospital, etc. but when I worked in the NHS many moons ago, it didn't seem particularly disproportionate to the size of the organisation. There were many more problems with people not doing their jobs properly but that was everyone, not just this nebulous "middle management" that everyone likes to cite!
Certainly, some hospitals under-perform and have issues with culture and discipline but that's the same as any business.
> Both underfunding and overfunding can cause inefficiencies, there is a sweet spot in the middle where an organisation would be at its most efficient.
I can't help but think that efficiency should be a secondary metric when it comes to health care. If you can get the same treatment, capacity, resilence etc. cheaper, go for it – sure. But as soon as you start to save money by sacrificing those more important metrics the price will be paid in human lifes eventually.
Every society has limited resources that it can afford to spend on healthcare, regardless of whether that funding comes from public or private sources. It is simply impossible to deliver unlimited, high-quality care to everyone. So, if we want to do the greatest good for the greatest number of people then the only option is to maximize efficiency.
> It is simply impossible to deliver unlimited, high-quality care to everyone.
Anything "unlimited" is impossible in a constrained physical world. So I am not sure what contribution you like to make by stating the obvious here.
For most economies delivering reasonable high quality care to everyone who needs it is totally a thing they can (and in some cases: do) afford. It is just a matter of priorities. You would be surprising what nations can sustain if they really want it. War is a good example. When a nation goes into a long war and changes its economy to support that war we call that a war-economy. It is an economy, that priorizes a lot of what it produces and outputs for the war effort. Nations can be years or even decades in war-economy mode without going under and that works because they priorize the nations existence (and thus the war) above other financial goals. And in war nations also make companies do things that would be otherwise unthinkable, e.g. make a company share blueprints with a competitor, favour certain industries with resources, etc. If any nation knows that, it would be the UK.
So if any modern western government goes all cheap and naive big eyes on health care, it is not because they can't do better, but because they don't want to. Not wanting to do better is a very easy opinion to have, especially if one earns money by being of that opinion. Those who suffer and die are also a different demographic than them, so even easier to pretend all is going well.
I am not saying that any health care system should be inefficient. It should be efficient in certain way (e.g. prevent funneling government money into pockets, prevent paying too much for medicine and equipment and so on). But efficieny is not the primary goal here, the primary goal is to have an adequate health care system. And you will always get unethical rich people saying private payer is adequate, because THEY are covered by it. But the fact of the matter is that everybody profits when a nation has a good working health care system for all, even the rich egomaniacs. After all they cannot decide where they will have a medical emergency as well.
Austerity IIUC is more about reducing the deficit than reducing spending.
Usually the way you achieve this is by reducing spending to reduce the deficit.
But you could also increase taxes.
Government spending will eventually be paid. It's whether it gets by the people now, the people in the future, or the bagholders (bond holders when the government or currency collapses).
Of course life expectancy is going to decline if you can't force your grandchildren to pay for your healthcare costs now.
But it's not clear to me that's the most evil thing in the world.
Back when most spending was infrastructure and growth was high, you could argue this would be around forever, and it should be financed to a large degree on future generations.
But now that a huge percentage of spending is entitlements and growth has slowed, it's less clear.
The thing about austerity, though, is that by reducing spending you also shrink the wider economy, reducing tax receipts. The "nation's credit card" rhetoric the government has used to try to justify this is just misleading.
In the case of the UK and NHS, under/overfunding doesn't quite capture the whole issue. The nature of spending matters, too. More spending on capital and managerial expertise could help improve things, but has largely been neglected due to political concerns regarding efficiency (or, perhaps, perceived efficiency).
The tl;dr here is that there's a striking number of patients in hospitals (up to 30% in some areas) which are ready to be discharged from hospital, but cannot yet be discharged since they're waiting for the availability of social services that aren't handled by the NHS. I've mentioned it in all my comments here but this is the cost of austerity, and it's making healthcare not just worse but more expensive.
The NHS is just a government department run by the UK Health Minister. Always point the finger at the person holding the purse strings and the person controlling the laws and policies.
The best time to start training more doctors and nurses is ten years ago. The second best time is today.
If only there were a decentralized system where consumers and service providers could allocate resources according to their value preferences by providing voluntary incentives.
You're referring to the US system of private insurers and healthcare providers which leaves millions without any access to healthcare and can result in bankruptcy as a result of an illness or accident? And which costs more per-capita for worse outcomes?
Pretty sure that is NOT what the parent comment was talking about. The US system has all the problems of a government run health system (which it basically is at this point) but none of the benefits. There are absolutely zero market dynamics at play in the US Health system any more.
>> leaves millions without any access to healthcare
Absolutely, 100% completely false.
>>can result in bankruptcy as a result of an illness or accident
This is true, however contrary to the social stigma bankruptcy can be a good thing for many. In the US Medial Bankruptcy is often made inevitable by various government regulations that prohibit creative solutions by providers.
Ok I'll be more specific: "leaves millions without insurance and since they're usually low-income and therefore cash-poor, unable to get any adequate access to healthcare". Is that really, meaningfully any different from what I said?
I have to say, the words "bankruptcy can be a good thing" is going to be bouncing around my head for a while. I don't know how less regulation could help these people, and I'm a little bit horrified thinking what kind of creative solutions these providers would come up with ...
>Medicaid is the largest source of funding for medical and health-related services for people with low income in the United States, providing free health insurance to 74 million low-income and disabled people (23% of Americans) as of 2017,[3][4][5] as well as paying for half of all U.S. births in 2019.[6] It is a means-tested program that is jointly funded by the state and federal governments and managed by the states,[7] with each state currently having broad leeway to determine who is eligible for its implementation of the program. As of 2017, the total annual cost of Medicaid was just over $600 billion, of which the federal government contributed $375 billion and states an additional $230 billion.[6] States are not required to participate in the program, although all have since 1982. In general, Medicaid recipients must be U.S. citizens or qualified non-citizens, and may include low-income adults, their children, and people with certain disabilities.[8] Along with Medicare, Tricare, and ChampVA, Medicaid is one of the four government-sponsored medical insurance programs in the United States.
>>"leaves millions without insurance and since they're usually low-income and therefore cash-poor
This is still false, infact the most impacted group by medical costs is the Middle Class not the poor. People too "rich" to be on public assistance programs like Medicade but too poor to afford a medical emergency and work for employers that either do not offer insurance, or have poor coverage.
>>the words "bankruptcy can be a good thing" is going to be bouncing around my head for a while.
I have known more than a few people that have gone through bankruptcy and it was the best thing they could have ever done. One mistake people often make is waiting tooo long to declare bankruptcy. Bankrupcy is a legal tool designed to provide aid to people who find themselves in too much debt, there are all kinds of things built into that system to assit people. It really is not a punishment. For example most people do not realize that they can Keep their primary residence and primary transportation even after declared Bankrupcy. People have this vision that is you file for Bankrupcy *protection* the police are going to come take all your things and put you on the street.
>>I'm a little bit horrified thinking what kind of creative solutions these providers would come up with ...
One thing that is prevented by Regulation is Medical Coop's several have been tried but they can not navigate the regulations to make them workable. Non-profit Member owned Coops would be a great thing for medicine, just has it did for Utilities in many regions of the US.
When even companies like Walmart can not make low cost medical services work directly as a result of regulation you know there is an issue.
You're dancing around the issue: you shouldn't need to have that debt, regardless of how spiritually cleansing you think the bankruptcy process might be. If you'd asked the people who went through it whether they'd rather a national insurer handle , I am sure they would have far preferred that. I'm quite shocked you know multiple people have had this kind of medical debt and can still come back with the bankruptcy-is-good-actually line.
I kind of feel like you're trolling me a bit, if I'm honest.
Or I guess I should ask what other requirements of life should be completely under the governments control? Should Government run farms and give you food for free? Should government build homes and issue them to people?
I have never been clear why healthcare is uniquely something that must be provided by government but other things are not.
If you think the government should provide everything you need to live like they were a parent or nanny well then we have completely and incompatible views as to what a government should be
> Should Government run farms and give you food for free?
The government do provide assistance for food for those in need, and they are right to.
> Should government build homes and issue them to people?
Local governments in most developed countries build homes and issue them to the needy. And I believe this is correct.
You've obviously deployed exaggeration to try to make these things sound ridiculous ("...completely under the governments control..." and "...live like they were a parent or nanny...") but really none of this is controversial, they're pretty common, mainstream beliefs.
I believe that a government should work to better the lives of the citizens it governs. This includes things like providing education, healthcare, road and rail infrastructure among other things you probably wouldn't like. I am quite sure we have incompatible views as to what government should be and that we both believe the other's vision of an "ideal" country would actually be a dystopia. However some of the happiest, healthiest and best-educated countries operate pretty close to my ideal.
>>The government do provide assistance for food for those in need, and they are right to.
This is always the comeback to that question. The US provides food assitance and Medical Care Assitance to low income people via many many many government programs, very expensive government programs
That is NOT the same thing as NHS, which completely takes over and provides the care. Food Assistance gives people with out income money to go buy the resources on the open market. Medicade gives people with out income money to go by resorces on the very regulated US health system
This is not an analog to NHS or other government run single payer health systems
So again I ask, not about providing social safety net, but should the government completely take over farming and housing like the NHS and other government provided programs do for health services
>>This includes things like providing education, healthcare, road and rail infrastructure among other things you probably wouldn't like
Correct, Government is incompetence personified. The incentives for government programs do not include providing quality services at the most value. Driving on my roads, going to the government schools I went to, and seeing first hand what "government housing" is has cemented the fact that government provides poor quality services at extremely high costs
>>However some of the happiest, healthiest and best-educated countries operate pretty close to my ideal.
That is very debatable, and not really supported by hard data
> That is NOT the same thing as NHS, which completely takes over and provides the care.
There's loads of reasons to dislike NHS care and it's genuinely weird that people who are so against the NHS never manage to hit on something real, and instead resort to stuff that's simply fiction.
NHS England spends billions commissioning care from private providers. That's why we have Priory Group, Cygnet, Operose, etc etc all providing care. (And in the case of cygnet and priory, often poor quality care).
And patients have a right to chose where to get their care - that's what chose and book is.
People who don't understand the NHS think it's a single organisation -which is what you've done here- and that's not correct. Patients have a choice of where they get elective care. NHS England commissions specialist services, and 42 ICSs commission the bulk of regular services. They're not allowed by law to have a preference for NHS providers, so if a private provider can do it for the money they should put a bid in. That commissioned care is provided by about 200 - 220 NHS trusts. NHS Trusts include ambo services, acute hospitals, community hospitals, mental health care, and community care. These NHS trusts are independent organisations that have their own boards of directors and their own accounts and they can compete against each other to provide services to particular regions. This does not include primary care which is provided by GP surgeries.
So the criticism here is when talking about "The NHS" as a free-at-the-point-of-use system, I didn't also go into variety of contractors that are now involved and specifically the NHS Trusts that exist in NHS England which I have never encountered having spent 25 years of my life in Scotland so I can't really talk about personally?
And how exactly would that have improved this discussion with "phpisthebest" who seems to be against the very idea of insurance altogether, given that they have the means to take care of all their healthcare needs in cash (for now), and who thinks that everyone else should really see bankruptcy as a sort of spiritually cleansing and enriching experience?
> This does not include primary care which is provided by GP surgeries.
Which are and have always been private businesses operating as NHS contractors - this was actually the concession the post-war government had to make in order to get the British Medical Association onboard with the NHS. And recent surveys indicate GPs are against any change to their private status.
Ok fine I didn't realise you were trying to lay a couple of little heffalump traps, so instead I just answered what I thought made sense. The given analogies are clumsy and don't really fit ("run farms" is silly - the NHS doesn't produce all of the things involved in the provision of healthcare - medicines and such) but I will humour you and answer in the context of the UK:
> Should Government run farms and give you food for free?
Probably not, the existing system works ok enough. They can maybe help the poor a bit more so they're not dependent on food banks (free school lunches was a recent controversy that shouldn't have been)
> Should government build homes and issue them to people?
I answered and you didn't like this but - yes and they should build more. I'll give you a little bonus and answer what you wanted to ask - "Should the government be the sole central authority providing housing?". Probably not, the housing market works ok enough in general. However they can maybe help the poor a bit more by building more council housing, not doing so is has directly contributed to making housing unaffordable for many.
And to bring us back to the original topic:
> Should the government have setup a national healthcare system back in 1948?
Yes - in the wake of WW2 there was no existing, competitive alternative that served the needs of providing quality, affordable healthcare to the populace. The NHS went on to deliver and then some. Plus with ~70 years of hindsight we see that in spite of a decade+ of brutal austerity, the NHS still costs less and delivers better outcomes than privatised systems like the USA has. It was the right thing to do, it is the right thing to do.
Also you seem to think they’ve shut out private providers altogether. This isn’t true, private healthcare exists if you want quicker access to some elective or non-urgent procedures or treatments.
Re your final point - this is very interesting. I'd like to know what countries you think I'm talking about, and if your libertarian (I think I'm right in saying this?), small government setup is anywhere close to implemented somewher right now or if it's purely theoretical/fantasy.
> If you think the government should provide everything you need to live
If you're going to argue against fundamental human rights like "right to life" then you're going to have to do better than the arguments you're using here.
Perhaps virtually everyone has access to health care, but certainly millions opt out at the cost of their own well-being because they can’t afford it. There have been times in my life when I have.
People opt-out for a wide range of reasons, Take myself as an example. I largely opt out of care even though I have great insurance, and ample resources to afford it even if insurance did not cover it.
My reasons for opting out have nothing to do with finances, it would get exactly the same amount of care if it was free.
Exactly, both systems are imperfect, but I'll take the half functional one over the inhumane one that also discriminates and ruins people while making excessive profit.
No, I'm not sure why this set of false alternatives keeps popping up. There's no need to read those implications into the comment. It was succinct and to the point.
Your comment hinted at a solution and I gave the closest example that most of us know - the US marketplace of private insurers. If you didn't want people guessing you could maybe have been more precise.
You don't want it to be a free market. People who need urgent health interventions are not ordinary rational consumers. They may not even be conscious.
Combine this with providers incentivised to provide as much healthcare as possible at the highest possible markup, and insurers incentivised to deny as much care as they can ... and you have what always looks (from the other side of the Atlantic) like a gigantic life-and-death financial nightmare.
Decentralised systems have a horrible truth: they tend not to optimize for the problem they are set up for but for the thing that creates the greatest feedback loop. In case of a healthcare system inside a capitalist society, the system will optimise for profit maximalisation, this automatically means that a large group is cut out of care because:
1) they require too much care
2) they cannot bring enough money to the table
Its a simple fact of how markets work. A free market is just an ideal, just like democracy, open borders and justice. It is not some law of the universe. In fact: countries that profit most of their markets are countries that highly regulate them. These countries include the US, China, South Korea, Zwitserland, Norway and Dubai. But not: Mozambique, Venezuela, Sudan, Russia, Haïti. <-- these countries dont have functioning markets because there is too much unregulated behavior, too much corruption.
Wait you are honestly claiming that Venezuela is captialist nation? Really?
The once shining example of Socialism that has now collapsed as socialism always does is "capitalist" now that it has failed? that is rich right there.
Russia is more or less the same... A Collapsed socialist state that never really adopted free markets, sure they adopted some aspects of capitalism but only because after the inevitable collapse of socialist policies the people in power divided up all everything of value between themselves and their friends. That is not capitalism either.
Free market is from the liberal ideology, and is like "well separated market with rationnal actors will take the most appropriate decision according to available information automatically". Basically.
Capitalism however: "an economic and political system in which a country's trade and industry are controlled by private owners for profit." And this is the Oxfor dictionnary definition because i don't want to misconstrue or be accused of bias.
I don't see how one replace another, in any situation. Sorry. You can very well have free market in a socialist country. More than that: in an anarchist country (which doesn't and would never exist, this is more than highly hypotetical), free market is the default and would need fewer regulation, as power in a market couldn't be leveraged to gain advantages in others.
>>. You can very well have free market in a socialist country.
you literally can not.
Free markets are one form Capitalism, All Free markets are Capitalistic, but not all Capitalist Systems are Free Markets. Other Capitalist non-free Market systems include things like Corporatism, Welfare State, Oligarchic, etc
Fascists are very often proponents of "the third way". Not saying you are a fascist, just adding some context to this. A little guilt by association.
I think the problem with the "third way" and with "communism" vs "neo-liberalism" is that they are all not focused on anything it's just a way to create a new "tribe". Conservation of Nature and worries about environmental decline used to be an elitist right wing conservative topic. Now its a leftist topic. Its not really about the topics, its about drawing lines in the sand and saying: "We from the left/right/third way, stand firmly behind this line! Who is with us?"
It is just a way to define a group that can be used to gain power.
It is easier to distinguish between laissez-faire and the ideologies you listed. For me this seems to be a more meaningful distinction. Especially as it relates to the topic at hand. Central planning comes into play where the market is not allocating resources. Fallible men with imperfect information vs. aggregated price information.
Putting back the percentage of GDP that has been deallocated for the NHS would go a long way to solving the issues that were caused by the deallocation.
That seems pretty uncontroversial.
There is, however, a large contingent of private companies profiteering from this situation; as the NHS was forced to buy things from private hands.
More money will not fix this mandated profiteering.
Do you think we should have more doctors in the UK? You are aware of the bottlenecks preventing that from happening? Do you think that it's just a question of money?
Literally right now it’s being reported that 300-500 people are dying weekly just because of extreme delays to emergency medicine. It doesn’t take many years to rack up 120k deaths at that rate (though I recognise the study was prior to this collapse and references primarily more diffuse causes)
I posted a years ago about how austerity was an outcome of the misuse of Excel for problems of scale that it wasn't designed for. Once some researchers figured out the problem with the spreadsheet that these governments were using, almost all stopped with austerity policies, but the UK didn't.
I posted that there would likely be one of two outcomes - a lost decade, we'd be in a worse position and no one should ever again think that the Conservatives are economic masters compared to Labour again, or that George Osborne was a bona fide economic genius and the UK would come out of this extended austerity in a fitter and leaner state ready for the challenges ahead (ala early Thatcherism).
The answer is the the first one - we had the lost decade, are looking at potential second lost decade and we're now equivalent to a central European country not France.
The Conservatives deserve to die at the next general election for this and should be replaced by a completely new right of centre political party as the opposition.
Unrelated to the main article, but I do find it quite upsetting that the Liberal Democrats have been absolutely crucified by both the Conservative party and the Media.
I can't go very far in a discussion about the liberal democrats without hearing that they didn't follow through on a manifesto pledge.
Which is wild because in a minority government, where you're given the option of electoral reform or sticking to another manifesto pledge; you have to pick one.
You're a minority government! You can't do terribly much.
Then the most recent leader of the lib dems being crucified publicly for being religious in some manner, (tbf: he said "I think Homosexuality is a sin but I support equal rights; and everyone should live free and with dignity")
Yet, the Conservatives do much worse and face no indigence in votes.
It's baffling.
FD: I'm not terribly supportive of any particular political party, but Liberal Democrats is one of the "more supported" ones of mine, along with SNP and Greens.
I assume by ‘breaking a manifesto promise’ you are referring to backtracking on the student loan issue. For context, the Lib Dems ran a campaign, the most talked about point being that they would get rid of student loan fees which had recently risen to £3000, the highest they had ever been. Not only did they not do that, within about two years of office they signed off on doubling that amount by 200% to £9000 tuition fees. For the average student, University tuition now costs even more than America (I can provide a source if you don’t believe this), and I would argue that the quality is nowhere near as good.
I voted for them on the basis of that pledge and I have never felt more betrayed by a political party in my life. It sickens me to my stomach. In this country you can only get four years of loans for university. I ended up dropping out of university because I was a mess in my late teens/early twenties. It means I now only have two years of funding left - not enough to get a degree unless I do a two year fast track course which are only available in certain subjects and of questionable quality. To go back, I would have to find a spare £9000 out of nowhere plus living costs which are most likely at least another £9000. This is particularly difficult when you can’t access high paying jobs because you don’t have a degree.
I’ve long since sorted myself out but I am now effectively priced out of bettering myself in my own country, directly as a response of the decision of this Lib Dem government. I taught myself to code to finally escape the minimum wage job trap. I have also been teaching myself Spanish over the last few years and I am seriously considering moving to Argentina or another Latin American country in order to access the affordable education. I am also going to start teaching myself German to open up the option of staying in Europe as the university costs there are minimal or free. Once I leave, I am planning on never coming back if I can help it. I feel that betrayed by my own country and have zero faith in it as a democratic representation of its citizens.
The Lib Dems could absolutely have not voted for that issue. They could have walked away and dissolved the coalition government. They chose not to. Well, decisions have consequences as I found out the hard way. And as a result, I will never vote Lib Dem again so long as I live.
> And Labour invaded another sovereign country illegally and set a lot of the groundwork for this current problem of the NHS having to continually sell its assets (such as real estate).
Yes I don’t agree with the Iraq war. But Labour didn’t run an election campaign based on not going to war in Iraq before getting elected and then going to war in Iraq. Or in the case of what the Lib Dems did, going to war with Iraq plus another two countries on top (200% increase). Iraq had no part to play in the election. I can’t comment on the NHS part because I don’t know specifically what this ground work is you’re talking about.
> And the Conservatives are the ones who actually instrumented those policies you dislike.
This is bullshit, it was a minority coalition government, if both parties didn’t vote for it it wouldn’t have passed. The Lib Dems are equally as responsible as the tories.
> Lib Dems went for electoral reform in the gambit of making it a more representative democracy; a gambit which lost.
This is one take. The other is that the Lib Dems voted for what was in the best interest of the Lib Dems (had they have won) and dropped all their other principles and pledges to the people that voted for them.
All the parties are rotten but as I say, I will never vote for the Lib Dems because of the direct consequences their decisions have had on my life. And I don’t think that makes me a hypocrite.
Electoral reform has been central to the Lib Dems plank since they first formed, of course they were going to go for the one shot at it they were ever likely to get. I was pissed off with them at the time as well, but in hindsight I was pretty ignorant of most of their platform at the time, which meant it was my unrealistic expectations of them that were broken, nothing more.
Electoral reform was also an advertised manifesto pledge. A pretty huge one actually: "a fair deal by cleaning up politics".
My key point here is that, while I understand you feel betrayed, the other parties are quite literally breaking their pledges left and right.
The main difference is that it seems to get not that much media attention.
That you wouldn't vote for someone who made a compromise against their values: but might vote for a purported anti-semite[0] or an actual racist homophobe[1] is disquieting.
[0]: Corbyn being accused of being an anti-semite is of course a load of tosh spun by the right wing media machine
> The Conservatives deserve to die at the next general election for this and should be replaced by a completely new right of centre political party as the opposition.
Important to note when people talk about "austerity" they don't mean cuts, but cuts in the future proposed spending increases. Public spending rarely goes down in absolute terms. Even as a percentage of GDP it doesn't really go down and certainly not since COVID
I dont know how big of a driver this is tbh. It seems more that a lot of people committed (publicly) to opinions and are unwilling to even consider to have incomplete, or even wrong views.
While in practice the overlap to toxic positivity is likely large, i think it misses that the cause is likely emotional/ego driven. So that people arent so much attached to positive narratives but their narratives?
Or what do you think the causes are?
edit: Never mind, should have just googled for toxic positivity. Thanks for the term!
Wrong. This has nothing to do with NHS because a similar surge of mortality has been seen in other countries. Surprising the BBC journaliste didn't think of checking this out.
Do you have peer reviewed evidence that lockdown is responsible for the excess deaths and not - for example - a deadly virus that happens to have been ripping through the population?
> Do you have peer reviewed evidence that lockdown is responsible for the excess deaths and not - for example - a deadly virus that happens to have been ripping through the population?
The article literally talks about this, and it doesn't seem directly related to COVID. Part of it is no doubt delayed diagnoses which led to terminal cases, inability to get care for mental health, and overtaxed and underfunded health systems.
I don't need a "peer-review scientific study" or "50year-long statistical study on 10,000 people", and then a peer-review to review the peer-review, to know that if you can't go to hospitals for 2 years, you'll be more ill as a result.
120k is "meaningless" if you do not mention how large of a population and how long of a duration - and the comparison that you do use is basically "clickbait".
And if you do not compare it with other causes of death, someone that doesn't deal routinely with these numbers (so, most people) still has no idea how much of a problem it is. (For instance I've been comparing war deaths in Ukraine to roadkills in Ukraine to gauge this.)
> 120,000 is a large number. It's approximately half of the entire city of Aarhus (Denmarks second largest city).
That's a terrible comparison though. In the US, about 3.3m people die each year. That's almost 60% of the total population of Denmark. A Denmark dies in the US every 18 months.
But that's just what you get when you compare a city with the population of a country that is a hundred times its size.
EDIT: Decide to swap the examples to British cities, inkeeping with what you said about apples/oranges; which people may be less familiar with; but hopefully it gives the sense of scale.
Sorry, I didn't mean the comparison to be a problem because Brits aren't familiar with Aarhus, but because I doubt the usefulness of this type of comparison.
"It's a large number" isn't useful when it's a percentage of an even larger number. ~1% of people die each year. Larger cities or nations will obviously have higher absolute numbers -- but what does that tell us besides that more people live there? If you can't visualize 120,000, can you visualize 67,000,000? Would "We'd losing a population the size of Aarhus if our population was the size of 100 Aarhuses" really make things clearer than saying "about 1% of the population dies in any given year"?
There are a total number of people who have died who wouldn't have otherwise.
It's not about "what is the delta" it's about imagining a literal city full of people who have died prematurely.
In terms of absolute numbers, "7%" is high, but not enough to really evoke any emotion in the reader.
How would you prefer to convey emotion to the fact that people's family members are no longer with us because of an economic policy which doesn't actually save the country money and has more in common with religion than economic science.
> It's not about "what is the delta" it's about imagining a literal city full of people who have died prematurely.
That's the thing though, there's always a city full of people who die, and it's pretty much always prematurely if you ask anyone that cared about them. There's no reason to help people visualize the actual number because the actual number is irrelevant. Would a 7% increase in the death rate be less shocking in Denmark even though it'd just be five villages and not half a city in absolute numbers?
Looking at absolute numbers to visualize things that are relative confuses people, because you'll need to play weird games when you want to get your point across but your population is 5m. "If we had 50m citizens, this would be half a city" is weird, people will rightfully say "but we don't, what are you talking about?"
I don't believe news should be aiming to convey emotion, or be manipulating. I also don't believe that the "how many football fields is that?" approach to news is useful.
I'm surprised it's not fentanyl. I work at a homeless shelter and there isn't a week that goes by when I'm not either trying to recessitate a client who has overdosed or finding their dead body.
It's an epidemic, and it's killing males and females who should be in the prime of their lives.
Yes and no. More people are also having more health issues because of a weakened immunse system (due to prior COVID infections). The "direct" link might not necessarily be made, but there's definite increased mortality as a consequence of COVID policies.
This is absolutely possible, alongside difficult to test and disaggregate for realities of post-Covid and long/chronic Covid sequelae that aren't even on the health quant analysis radar for the most part, despite the wealth of mechanistic and stochastic dots that remain unconnected, at least in official public utterances.
“The vaccines are a success… but you need to take more vaccines to be protected”
Surely you can see that the goal posts have been shifted from the days of “the vaccine is our road back to normalcy” and similar mantras when they first were pushed?
It was originally touted as the solution. Many people who were silenced, fired, or worse, were silenced from objecting with the idea that “this isn’t a solution, I’d rather not”
And now we’re saying it was a rousing success, yet it isn’t enough at the same time…
Hard to be sure, but I would suspect very probably, although perhaps not for that reason.
Long covid is real, and statistically significant. Heart and blood stream involvement issues with covid have also been apparent from the start. Put that together and any uptick in heart attacks, strokes, etc. might well be longer term consequences of Covid, and put that together with overloaded health systems, and not just in the UK.
> likely to have been driven in part by activities in response to the coronavirus (COVID-19) pandemic, such as testing and tracing services and the implementation of the vaccination programme
So probably no increase, pandemic billions are gone and no one will see them again
The rest service itself probably had a cut with the inflation, and increased processes and bureaucracy to manage
Now that the BBC has mentioned it, is the Govt going to do a proper investigation of why and do something to fix it?
Covid, Covid vaccines or not, excess deaths should be falling because the excess deaths of previous years should mean a deficit of excess deaths in the following years.
Something has gone deeply wrong and the Govt is doing nothing and leaving the underlying causes to BBC speculation.
These figures should also be analyzed properly by age group, something the BBC journalists are clearly not interested in even though they have the resources to do.
Hey, it's absolutely not true that the government is doing nothing. They're actively cutting the pay of Nurses, junior doctors, ambulance workers, and emergency services call handlers. This has resulted in a series of strikes further destroying the service as well as causing a recruitment crisis. In response the government is planning to pass legislation to ban strikes that will allow ministers to ban strikes in practically any profession - from tram drivers to the passport office to nurses to border guards. In response to this legislation there will be a general strike, probably causing the government to collapse.
I looked into normalized deaths per capita a while back, sometime late/post pandemic. What was oddly fascinating for me to see is the figures in the early 90s were actually a tad worse than during the pandemic. But progressively since the 90s the death rates have been consistently improving, bar covid.
Of course this data reflects the actual lockdowns experienced and not any what-if of the impact of death rates if we continued covid without lockdown.
Smoking has dropped from around 55% of the population in the 60s to around 13% now. It was always one of the biggest killers, and as smokers died out and smoking became unfashionable life expectancy - unsurprisingly - stared to improve.
Last time I got heavily downvoted for this, but please if you're in the UK do not rely on the NHS. Indeed, you cannot rely on the NHS. There is no knowing whether or not they will have the capacity to save you.
You probably got downvoted because there is literally no alternative (except perhaps being airlifted to a different country). The NHS is basically the only provider of emergency care.
My Great Aunt in Scotland had the flu, which was so bad she had chest pain. She went to her GP who told her to go to A&E. Even with her GP informing the hospital she was coming, and that she had chest pain it took her 14 hours to get a bed.
Absolute madness. The system is bursting at the seams. It appears that the UK is breaking apart in so many different ways; the budget, health system, education, etc.
I'm not sure a change of government will solve all of this.
something I keep seeing in the comments. is people blaming the gvt for not training more doctors. and yet keep forgetting that students have to incentivized to train as doctors i.e there has to be hope for better pay, better working conditions which are currently not on offer right now.
so the smart kids, who might have chosen medicine chose other fields. economics at play - allocation of scarce resources.
the only thing that keeps NHS humming in terms of doctors / nurses is due to those professions being recruited from 3rd world countries.
One day the world will wrap its head around the fact that having COVID affects your immune system long-term and as such is bad for future health outcomes.
Yet with 80%+ (or so) of the population vaccinated, one would expect a drop in people dying from covid
At least - that’s what they said when it came out and they demanded everyone take it.
Plus with all the boosters, combined with the general trend of dwindling intensity of viruses in a population over time, one should expect this effect to be even more dramatic
Yet here we are, talking about covid like it’s April 2020. How it’s so devastating of a virus, like we’ve gained nothing in fighting it since then
Funny how literally any metric can be used to justify covid madness
> type of Covid vaccine has been linked to a small rise in cases of heart inflammation and scarring (pericarditis and myocarditis). But this particular vaccine side-effect was mainly seen in boys and young men, while the excess deaths are highest in older men - aged 50 or more.
Alternative explanation. You only see the heart inflammation in young men because its unusual. In older people you already have it because of age so extra inflammation could go undetected.
Why COVID-19 is considered to be a respiratory disease
Medical professionals and researchers have been studying the link between COVID-19 and vascular symptoms since the beginning of the pandemic [..] These observations led to several hypotheses that COVID-19 was a vascular disease with respiratory symptoms and not a respiratory disease.
Studies in 2020 and 2021 supported this theory. These studies concluded that although people with mild to moderate COVID-19 only had respiratory symptoms, COVID-19 was primarily a vascular disease. However, additional studies published later in 2021 and into 2022 have contraindicated these findings. New studies indicate that COVID-19 doesn’t attack the vascular system at all.
"Finally, figures up to June 2022 looking at deaths from all causes show unvaccinated people were more likely to die than vaccinated people.
While this data on its own can't tell us it's the vaccine protecting people from dying - there are too many complicating factors - if vaccines were driving excess deaths we would expect this to be the other way around."
What a shitty article. No mention of the cuts to the NHS by the tories and the effect that had on its ability to serve the public but they make it seem like this is a side effect of the covid vaccines? What the actual fuck.
Spending on the NHS is increasing a rate that is below the rate of increase in demand (the gap is about 3% year on year IIRC). Informally you might say this is a cut. It's easier to communicate to an unsophisticated audience.
I guess you can restate "cut" to suit your point. I'd even accept "cut" if it was less money in real terms (i.e. after inflation). But I don't think you can define "cut" as "not giving the NHS all the money it asks for, even though it got more than last year".
You can pedantically argue whether this is a "cut" or not, but that's not the issue. Nor is the issue how much the NHS asks for. The issue is there is less money per health-care-incident to provide care.
> this is likely to have been driven in part by activities in response to the coronavirus (COVID-19) pandemic, such as testing and tracing services and the implementation of the vaccination programme.
Yes, if we include the many billions spent on faulty test and trace and broken PPE -the corrupt spending that went to pals of the Tory party- we see an increase in health spending.
Guess what happens to the amount of health care funding if you ignore the corrupt spend on PPE?
One area that I think is interesting to look at, aside from overall budget, is bed capacity and nursing staff numbers.
According to Statista:
Bed capacity is significantly lower than at the turn of the century, but more damage was done there by Labour than the Tories [1].
The numbers of nurses has steadily increased in the last twenty years under both Labour and the Tories [2].
So if there are many more nurses per bed than there were twenty years ago, why is patient safety one of the issues they are currently in dispute with the government over?
I don't know the answer to this, but I think we need to know. It is, like teachers, that nurses are spending so much time on non-clinical bureaucracy that the don't have time to nurse?
You reduce bed numbers by pushing less sick people out of hospital. This means that your two 6-bed bays now don't have 4 people who need minimal nursing, 6 people who need moderate nursing, and 2 people who need high level nursing. It means you have 8 people who need moderate level nursing and 4 people who need high level nursing.
There is no NHS in France or Germany, yet, the same phenomenon is observed. So, yes, deal with it, the common point is the COVID and the lockdown. Does it really require a high IQ to understand that closing hospital and doctors appointments for 2years will result in undiagnosed/untreated diseases ?!
This is not just an UK phenomenon though. You can find reports from countries from all the continents, except for Africa. It seems they fared the best in the last 3 years notwithstanding all the apocalyptic news headlines in early 2020 predicting a blood bath once Covid reached them.
Another possibility is that Africans have better immunity due to, uhm, natural selection? The human body has its own mechanism in defense which is more sophisticated than any of medicines out there. Natural selection is also how we came out to be. I think it was foolish to think that we can do better than a hundred-million year of a refined process.
The above comments are several dumb takes. Also, reports are not the same as actual outcomes. The buck stops with excess mortality.
In my visits to Africa since the Pandemic started, they are taking COVID quite seriously, with lots of measures against it. And not ignoring it at all (1).
Ironically for your assumptions, this may be a result of cultural selection: this isn't their first infectious disease to deal with as a public health issue in living memory. Not to say that there's no COVID there, people are still getting it, people that I know there have had it, varying number of times with varying severity.
1) YMMV, Africa is vast, I only visited one corner of it. Blanket statements about "Africa" are false somewhere.
"Finally, figures up to June 2022 looking at deaths from all causes show unvaccinated people were more likely to die than vaccinated people.
While this data on its own can't tell us it's the vaccine protecting people from dying - there are too many complicating factors - if vaccines were driving excess deaths we would expect this to be the other way around."
It's simple math but anti vaxxers are consummate innumerates.
I've been double vaxxed and boosted, so I'm not an anti-vaxxer. I don't know for sure if the vaccine is causing more heart-related deaths. I do however believe the government (any government) would lie to get people to take a vaccine if they thought the number of heart deaths due to vaccine would be lower than the eventual number of COVID deaths without a vaccine.
If you mean Aseem Malhotra, he is an idiot and nobody in the entire region of London that he trained in thinks he has an IQ above 100. Pre-COVID he was unemployably bad as a doctor, and has never had a formal job in the NHS since he completed his training. He has latched on to vaccines hoping he can make a quick buck that way.
What is your opinion on Japanese professor Dr Masanori Fukushima [0]? He seems to think the vaccines are dangerous as well and here in this video he talks directly to the Japanese Ministry of Health (from my understanding).
Nowhere does this article suggest it is linked to vaccines. In fact there is a subsection in the article titled:
> No evidence of vaccine effect
The increase in excess deaths is a symptom of healthcare system that is being increasingly starved of resources and which is having to make up for cutbacks across various parts of local and national government.
It's about austerity, not covid vaccinations - let's not bring misinformation and conspiracy theories into this.
Not me, but you have no basis for the degree of certainty you are displaying.
For me this has become an exit criteria for serious discussions. Once you are overcertain i realistically no longer argue the actual issue but against you not wanting to have been wrong. As i see it, given my social competence, best case would be making you over correct in the other direction or make you cry. Both bad outcomes.
I would recommend getting to grips with the varying degrees of uncertainty of a complex world. I get that this feels bad, but simply betting on the frames that make you feel less bad, even just because it confirms your view, is not a winning strategy.
The chances of myocarditis are still much higher with actual Covid than with the vaccine. And given that Covid is endemic it's just a choice which immunization method you prefer Covid or mRNA.
Comparing the side effects of those two methods I think mRNA definitely wins out. Of course that's only the case if you ignore all the FUD being spread about how the mRNA vaccine will definitely kill you.
What are your chances of myocarditis if you're vaccinated and get covid? It seems like that would expose you to two sources of risk.
Also, the assertion in your comment is not true for all age groups. For males under 40 it has been repeatedly shown that the risk of myocarditis is greater from the vaccine (and increases with each dose) than from Covid itself. You are correct that on average across all age groups there is a higher risk of myocarditis from Covid.
> The chances of myocarditis are still much higher with actual Covid than with the vaccine.
Nope. That is only true if you were hospitalized for a severe case of Covid. There is virtually no myocariditis for short covid episodes where you recover quickly.
Right if you asssume your case will be mild then there is virtually no risk. There is also no risk from mRNA if you assume the vaccine won't give you any side effects.
There is one combination where the risk of myocarditis does come close to Covid-19 and that is with Moderna and men under 40. However myocarditis isn't the only potential side effect from Covid and you can just opt to get Pfizer instead if you're under 40.
You don't have to assume. You know it from almost Day + 30 of the pandemic that the people at real risk of a bad COVID were old and with 3-4 comorbidities. It was never a secret. The media has just been hyping up the risk to make it look like everyone could die from it for absolutely no reason.
This data has virtually no value because it is based on myocarditis that was diagnosed and detected and who knows how many goes completely unnoticed or undiagnosed. You can't compare the rates of rare events this way.
Interesting to look at the footnotes for disclosures too:
> A.S. is a member of the Scottish Government Chief Medical Officer’s COVID-19 Advisory Group, the Scottish Government’s Standing Committee on Pandemics, and AstraZeneca’s Thrombotic Thrombocytopenic Advisory Group.
> J.H.C. is chair of the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) risk stratification subgroup and a member of Scientific Advisory Group for Emer-gencies (SAGE) COVID-19 groups and the NHS group advising on prioritization of use of monoclonal antibodies in SARS-CoV-2 infection.
> A.H. is a member of the Joint Committee on Vaccination and Immunisation
Color me surprised that people whose livelihood depends on recommending vaccines and COVID19 treatment end up "finding" that vaccines cause less side effects than COVID19..
Even if the data is incomplete, it's the best we have right now. To the best of our knowledge the vaccine is the best option.
Of course there's a risk cases are being undercounted or there is some long term effect we just don't know about that goes against what we know about mRNA today. But that's life unfortunately, a chain of decisions based on your best knowledge at the time some of which may turn out to be wrong.
> Color me surprised that people whose livelihood depends on recommending vaccines and COVID19 treatment end up "finding" that vaccines cause less side effects than COVID19..
One of them serves on AstraZeneca's advisory board which is not an mRNA vaccine, in fact they would benefit from overestimating the risk of myocarditis with mRNA so the AstraZeneca vaccine would compare more favorably.
Another one serves on a board to prioritize the use of monoclonal antibodies, so he benefits from people who remain unvaccinated and get hospitalized.
If anything these people have a conflict of interest to inflate the dangers of mRNA vaccines.
> The media has just been hyping up the risk to make it look like everyone could die from it for absolutely no reason.
No argument from me there, but for anyone who thought the media wasn't prone to scaremongering hasn't been paying attention during the Ebola outbreak. However even if we are in a demographic not likely to have severe cases we shouldn't ignore the real strain epidemics put on the healthcare system and the risks it poses to demographics who are vulnerable. Also have you considered some of your own sources may be hyping up the risks of mRNA vaccines?
While the vaccine is available to everyone I prefer getting it even if I'm not likely to get hospitalized. Because based on the available data it looks safe enough to me and it gives me the option to plan some days off in advance to deal with the vaccine side effects rather than suddenly getting Covid and then having to deal with being out for a week or more and having to worry about additional side effects whose severity exceeds the vaccine.
> To the best of our knowledge the vaccine is the best option.
based on clinical data that nobody has seen apart from a few experts in the FDA who are probably paid by Big Pharma anyway.
Its funny, I remember not so long ago on HN when the prevailing sentiment was that Big Pharma was just right next to Satan in terms of evil, but suddenly after the pandemic hit it]'s almost impossible to say that their motives and their data should be questioned. People have been completely brainwashed and were too quick to forget about VIOXX, Oxycontin and a lot more
Intellectually weak stuff. The vaccines were far safer than the alternative (remaining unvaxxed), especially at a societal level, but like all medicines they carried adverse effect risks. If you want zero risk in your life - rather than tolerable risk for wider benefits - I wish you luck. Even eating food (which sometimes causes food poisoning!) must be causing you mental anguish.
He is suggesting that that vaccines had no effect on reducing spread, which they did not. They kinda like flu booster shot. Could maybe reduce symptoms, but we are not even sure of that at this point.
Vaccinating kids or anyone under 40 for that matter was wrong, period.
They reduced deaths from covid by an absolutely insane level, it's undeniable and easily provable. Without vaccines we would still be doing regular lockdowns.
Look at those first two massive spikes in daily deaths in the last two charts. That level of exponential increase in daily deaths led to two long lockdowns, which as you can see temporarily dealt with the issue. Can you spot where vaccines were introduced en masse and we never had a lockdown again? It's really not difficult to see that vaccines effectively stopped exponentially growing daily deaths. To argue that they had no effect is bordering on insane, or at least just extreme ignorance of data.
* To argue against lockdowns is to say it's perfectly fine for those exponential deaths to climb to the level of tens of thousands per day. Obviously no reasonable government was ever going to let that happen, it would be a PR nightmare. So the anti lockdown argument was always a non starter.
* To argue against vaccines is to say that it's ok to have regular ongoing lockdowns.
Yet paradoxically the anti lockdowns and anti vaccine crowds are the same! Frankly, both positions are completely silly.
(A reasonable argument could be made for no lockdowns, but the reality is no western government would ever implement that strategy. We have to live in reality.)
Because it’s so hard to understand the complicated math that is 50x — aka you’re 50x more likely to experience heart issues from catching Covid than getting the vaccine. If you think you can avoid getting Covid then you may have a point. But for any normal rational person living a normal rational life, the vaccine makes sense. I understand you may not fall into that group.
> aka you’re 50x more likely to experience heart issues from catching Covid than getting the vaccine.
This is completely false, because it cherry picks the data from people who were hospitalized with severe COVID cases. Most people who recovered with very few symptoms after COVID did not end up with any heart damage.
If that is "cherry picking" -- then your data is also cherry picked --- as people who have the vaccine are less likely to end up with severe Covid hospitalization
Is this really a mystery still? Well we know we can't blame it on fats anymore, our governments have tried that completely failed trope for 70 years now. And looks where it's gotten us. Heart disease is killing western diet eaters like there's really no tomorrow. I think it's obvious that constantly high insulin is the biggest driver of vascular disease. Hyperinsulinemia precedes diabetes and is measurable 10-20 years before your a1c will detect pre diabetes. This drives virtually all diseases of "modern western man/person" - heart attacks, stroke, dementia, connective tissue diseases, diabetes. It's insulin!
Low fat diets high in refined carbs disrupting the absorption of k, d, e, a. sugary beverages with zero fiber, 3 meals and 5 snacks a day so your insulin levels never come down even at night sometimes. Your body can never repair itself or stop storing fat instead of using them. 3 meals and 5 snacks a day= zero ability to distinguish cravings and real hunger. Being told to gobble 5+ fruits a day by every dietician. Fruits bear in the winter, we live in climate controlled buildings. Why are we gobbling so much fructose from 5+ fruits a day.
You're leaping to a conclusion that this is a problem with individuals' dietary choices while missing that the NHS has to do more with less year on year. Importantly while the former may be an issue, it is near-impossible to fix - encouraging healthy eating has been a priority for decades. Whereas addressing the latter should be very doable if the major parties agreed that adequately funding the NHS (and other social services) was a priority - sadly both seem to believe that a public-private partnership and more austerity is the way forward :-/
The only healthcare services that deliver a significant improvement to life expectancy at the population level are vaccinations, antibiotics, and trauma care. And those services are cheap. Everything else is pretty marginal. Diet and exercise have a far larger impact than almost any healthcare interventions.
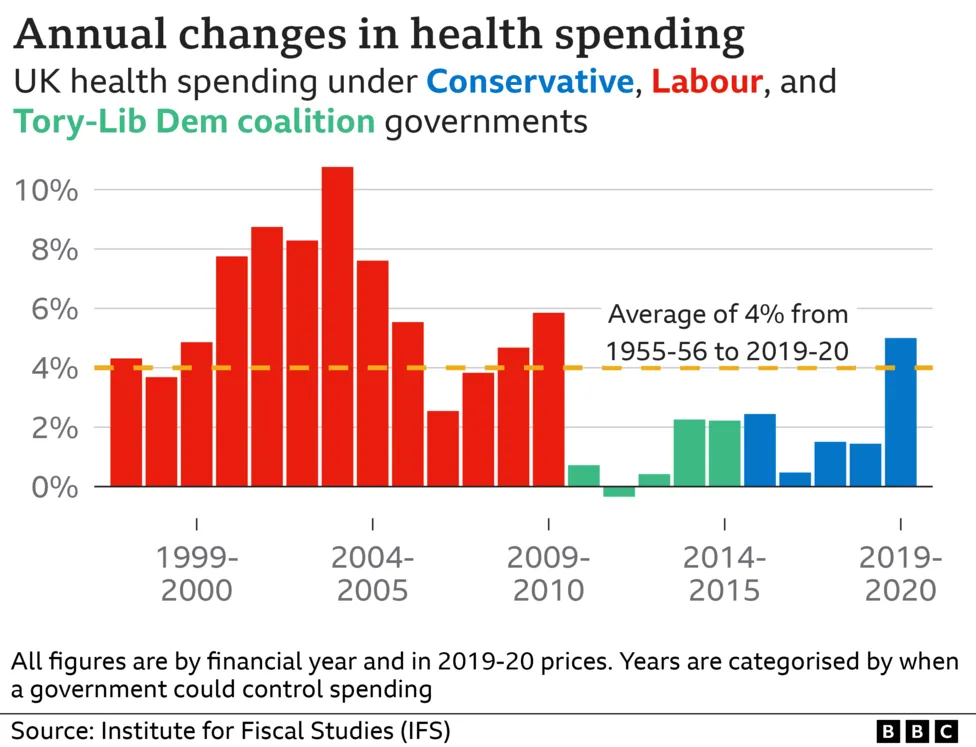{kind=link}
{kind=link}
{kind=link}
All of which I mean to say: No. Shit. Sherlock.
It's all so painfully obvious to anyone paying attention. The doctors and nurses and care homes and mental health workers have all been screaming about this for a decade. Cuts upon cuts upon redirected funding upon private providers upon universal credit cutting benefits upon cuts and failures and all that before covid, all before inflation lowering everyone's incomes.
We need to hire. We need to train. We need to retain. We need to build. We need to instill the fact that care home workers, pastoral carers for our elderly are such bloody important roles because without them helping people live outside hospital, nobody else gets seen. We need to pay them, we need to pay them to pick up shit and talked to dementia sufferers more than Jeff Bezos can pay them to pack boxes.
If we can't do that… It's over. But we need to have a serious conversation about what we actually want to do with the infirm in this country. Letting them freeze to death in their own homes feels like state-mandated euthanasia without the "eu". Huh, a wild Brexit joke appeared.
We need a General Election.