It is astounding to me how locked down certain medical tests are.
Like, if I want an EKG, why can't I just walk in to a place and get it done at a reasonable price? And without a doctor's approval?
And I pay for insurance. But I just want to be able to monitor my vitals myself, whenever I feel like it.
It seems like it would drive higher utilization of equipment and lower prices if these types of diagnostic tests were readily available at a place like a CVS or a Walmart.
I would gladly even pay $50 per month for unlimited access to a place to just come in, get my blood sugar, kidney function, heart function, liver function, etc. tested once per month!
As important as health is, and as much as Americans spend on it, it is shocking to me how gated everything is.
It hurts my health and my pocketbook simultaneously!
I've always wondered why a company like Walmart doesn't just provide $20 EKGs, and $25 tooth cleanings.
Like, why is so easy to get a hamburger at any time of day, but like pulling teeth to just run somewhere and get a quick, inexpensive EKG to make sure everything is ok with your heart..?
What am I missing? Are there legitimate safety reasons these mundane diagnostics are so locked down?
Or are these services available and I just don't know about it?
Again, I pay for health insurance, but I still feel like if I want a quick EKG, it will take me 3 weeks to see a doctor, and by then I might be dead. I don't want to see a doctor, I just want an EKG done for my own peace of mind.
But health Care is not my area of expertise. So perhaps there are very legitimate reasons these diagnostics and labs are so difficult to self-request at reasonable prices.
Medical tests can also be counter productive. Hear me out. There's studies that regularly show the optimal age for i.e breast cancer screening. Screening too early can cause an increase in misdiagnosis I believe. There are other such cases for not just cancer screenings - I know not exactly what you're talking about. EEG and blood test make sense. But for more advanced tests, you could be right in saying "there are legitimate safety reasons" - maybe not so much from the test itself but from the impact of a false positive.
I'm so fucking tired of this perspective. Yes, it's technically correct. Many of us have done the canonical "cancer screening false positive / false negative" example demonstrating the problem in a statistics class.
But at the end of the day, I'm paying a doctor to care for me, not the general public. I may be a member of the general public, but the public interest and my interests are not identical.
If I'm willing and able, I should be able to pay to have a test done (anonymously), and be left alone to deal with the statistics of what the results actually mean for myself.
The fact that I have to fight my doctor to do this is condescending bullshit.
It's a bunch of gatekeeping bullshit and drives me crazy. My wife went through two years of misery and the number of times I had to argue over getting labs done that ultimately influenced her treatment left me with a rather deep mistrust and skepticism over the medical community that is going to take a lot of time to repair.
The reason you don’t want to do “all of the tests” and “deal with the results” is not about the probability of a false positive, but the consequences of getting one:
“In the United States, estimated deaths per year include: [26][27][28][29]
12,000 due to unnecessary surgery
7,000 due to medication errors in hospitals
20,000 due to other errors in hospitals
80,000 due to nosocomial infections in hospitals
106,000 due to non-error, negative effects of drugs
Based on these figures, iatrogenesis may cause as many as 225,000 deaths per year in the United States”
This is exactly what the doctor parrots back at me. Again, these are outcome statistics for the general population. I'm well aware of these numbers, but I am not an average patient.
I'm not going to look at the outcome of a single test and blindly decide to take a strong medication or to get surgery. If I want a test done, it's because I'm doing research to try and figure out a complicated issue that doctors have not been able to help me with, usually due to their own time and resource constraints. I have all the time in the world, and if a condition is affecting me, I'm going to care more about addressing it correctly than any doctor. I'm completely aware that a test is just one data point, that tests have error rates, and that interventions have risks.
I was one of the first ~1000 to get whooping cough (pertussis) during the 2008 outbreak, before they knew that the vaccine cocktail that my generation was given needed more frequent adult boosters. I figured it out after a few days of digging. Do you want to know how many doctors I had to yell at to finally convince one of them just to run the test? And this is a test with zero intervention risk -- they can't do anything if it comes back positive, they just tell the NIH.
Doctors have gone off the deep end here. Yes, testing has risks, but they should focus on the intervention risks. You should be allowed to run as many tests as you want for informational purposes if you're just trying to figure out what might be going on, especially if you're aware that errors can happen and are capable of acting responsibly with the resulting (single, noisy) data point.
You might have a case if you were paying for the test out of pocket, but I presume you have health insurance. In that case, it is also the doctor's duty to prevent unnecessary spending.
Combined with the fact that most patients are not well informed and will demand pointless or even counterproductive, it is better to leave treatment and testing decisions to doctors, not patients. Even if doctors sometimes get it wrong it is still better than the alternative.
I'm not saying you shouldnt be allowed to pay and pick your own tests or your loved ones tests. You have a good point, population statistics can't be extrapolated back down to an individual on a case by case basis. I had to deal with doctors recently, so I understand where this frustration comes from. I only mean to say that there could be some negative effects from people doing this in aggregate.
You might change your mind if you'd ever met an arrogant doctor whose biggest concern was their own ego and you didn't have a second option. I'm met a few doctors who are so rude and arrogant they wouldn't even pass the HR screen at anywhere I've worked. Depriving people of choice just gives assholes even more of a chance to be assholes, because people have no other alternatives than to go to the assholes.
You're right - depriving people of choice can cause bad doctors to stick around longer because patients are forced to go to them.
This is why we need something like single-payer - no one should be forced to go to a bad doctor because their private insurance decided to only have one or two options in-network locally.
Yes, but that argument would prove too much. People get very anxious just from browsing medical information on the Internet and matching up their easily observable symptoms.
> I would gladly even pay $50 per month for unlimited access to a place to just come in, get my blood sugar, kidney function, heart function, liver function, etc. tested once per month!
(I agree with the other commenters that frequent asymptomatic blood testing is unlikely to help, even more so when done alone - not because of false positives, just because CBC results vary a lot for no detectable reason/problem)
Just checked the price on CBC from any lab test now, $50. That's still pricey for most people, especially for a half-dozen similar tests per month. Walmart has historically proven very good at forcing prices down through economies of scale.
No one without symptoms needs these tests every month. Meaningful changes manifest with symptoms or happen slowly or both.
As an example of the first case, a person’s white blood cell count isn’t going to go haywire overnight with no other symptoms. An example of the second case is fasting blood glucose: it's important to know before symptoms appear, but is not going to change dramatically (beyond the draw-to-draw/day-to-day variation) in a month, or even in 3-6 months.
Getting these monthly with no medical need is like telling someone you’re aiming for 300% test coverage :-)
It's a massive waste of money and resources to get an EKG without a clinical presentation. It's a massive resources to get a CBC and CMP without some positive predictive value. Why don't we throw every test at you? Because there's a significant chance you will be a false positive/negative. This is dangerous to look at this way.
What are those risks, like, what do they look like quantified?
"Waste of money and resources" is relative if you're only blowing ~$200 bucks. Even if there is a 8-10% chance of a false positive, they're cheap enough to do two... or 8. Kinda like how people by multiple cheap birth control tests.
Anecdote: I've had hernia problems off and on courtesy of the USMC and did no less than three (3) sonograms after being referred by different GPs to do so -- and they found nothing. Symptoms didn't go away and I kept going back. This was in the Inova system around Washington DC, one of the better systems in the US. One afternoon I double over in pain and end up in emergency surgery because, low and behold, I did actually have a hernia and it was strangulated; my intestine was literally dying one inch at a time. Emergency surgery saved my life, but I paid ~3-4K for all of those sonograms & consults + more for the actual surgery. All in maybe $8-10K.
Walmart-tier medical may not be great, but one of the better health systems in the US failed me just as effectively, and at a greater cost. Would 5 Walmart sonograms have found it? 10 scans? Maybe not, but I probably could have done 10 scans and still saved money.
If a test has 5% false-positive rate, you can't just test 5 times and expect to have a <0.000001 false positive rate, maybe not less than 1% or even 4% - depends on the test and how you repeat it.
If they test you for antibodies, and your blood reacts, doing the same thing 5 or 50 times is not going to help. If you have a wobble on your EKG, it's not going away just because you measure it 10 times. Though it might, if you were just stressed the first time. Or they might find something 2 out of 10 times and then what - do you just ignore it?
To be clear, I'm not against non-invasive voluntary testing, but procedures need to be adjusted, otherwise people get treatments they don't need and suffer the effects (while also tying up actual doctors and equipment).
BTW sorry about your issues. Those were false negatives, and you had symptoms, where better/additional/more tests are warranted.
Medicalidiot, the most an EKG machine costs is a few thousand dollars if that. Running the machine costs probably less than a penny in electricity. What is the "MASSIVE" waste of resources here?
Reading the EKG gets billed at $200-%300 because you want a board certified cardiologist who can look at the nuances of an EKG to tell you whether your right bundle branch block is part of the 99% that is likely benign or if it's that 1 in 100 that we are going to put you under intense therapy so you don't die.
Because it fell off everybody's radar, I assume CVS MinuteClinic hasn't been as revolutionary as originally hoped. OTOH, if Walmart is joining the fray then either the retail clinic market has been steadily growing in general, or Walmart thinks they can do something different.
I tried it once in 2007 and it was quite pointless. The person in charge at that location was I think a real MD but she appeared to be encumbered by hard policies that restrained her from pretty much doing anything. I regretted wasting time there since I had to go to a regular doctor anyways and haven't been back.
I've only ever used them for flu shots and a tetanus shot once. They're a perfect supplier of those kinds of services in my experience. I think if I were actually ill or something I'd try to bump up to the next tier and at least go to an urgent care if I can't get into my primary care physician.
Problem is MinuteClinic is just that, a clinic, it's just a nurse that can do "office treatments" such as vaccines, shots, prescribing blood tests, bandaging wounds, etc. But ultimately anything else has to be referred out.
Prescribing blood tests might already save doctors time. Most of the time when I'm sick the doctor just asks broad questions and takes a blood samples... and I'm told to come back tomorrow when the results are back from the lab.
This argument is comparable to thinking that a painting is only worth the materials it’s made out of, and everything else is worthless. A doctor and their staff have trained for decades in order to handle your health, why in the world do you think you can do it after some googling?
Compare it to your own job - if I had the same tools as you, could I walk in and do the same job you do?
>Compare it to your own job - if I had the same tools as you, could I walk in and do the same job you do?
Should access to a compiler be gated just because amateur programmers probably don't know as much as people with a degree?
The fact that you need to go to a doctor, to get referred to a facility which will run a test, which will then send that test data back to the doctor, and at the second appointment the doctor will go over the data with you to see if you needed to go to the doctor in the first place...is just an absurd waste. It shouldn't be so hard to get a few measurements done on your own body.
My point is that a random person with access to any highly specialized tool will not output usable results. If I try to use a compiler and mess up, nothing bad happens.
If I go get myself an EKG and mess up the reading, well.. death is somewhere in the list of possibilities.
(To be fair, I fall into the group of people who believe in very strong government regulation to protect people from themselves, because the world is too complicated to make well-informed decisions. Easy example is seatbelts - if Ford could sells cars for $1500 cheaper if they didn't have seatbelts then some people would buy them and they'd die. Not everyone will do the proper research, so everyone needs protecting.)
> A doctor and their staff have trained for decades in order to handle your health, why in the world do you think you can do it after some googling?
Counterpoint: Doctors have an average IQ of 115, and train across a huge variety of disciplines; mostly while sleep-deprived. Many doctors' training was decades ago.
Anyone with a somewhat abnormal condition, access to Google Scholar, and able to learn how to follow citations and simultaneously weigh competing models can outdo anybody except a dedicated specialist.
The relevant job comparison isn't to a painter, it's to a programmer with a hundred clients, each of whom he talks with for 30 minutes, once a year. Sure, the programmer has much more knowledge and skill--but is he really going to be able to adequately replace the every client's home-brewed solution spread across 4 excel sheets, 3 batch files, and an archived website?
Should the client really be restricted from downloading Python or Visual Studio for their own use, unless a real programmer signs off on the requirement and supervises them?
The variety of disciplines and sleep deprivation is only about 2 years early in the training. After that the training is highly focused, and again only 2 years or so are sleep deprived. And today, the majority of doctors in practice are less than 20 years from their training. You make it sound like doctors are an outdated mass of idiots, and I can only assume your personal experiences have biased you.
The real training is objectivity, which is very difficult for even doctors to maintain, despite knowing just how misleading research results can be and so how they must be wary, how to rationally follow the literature, etc.
I seriously doubt more than single-digit percentages of people googling things, even intelligently, are going to be following citations and weighing competing models. Likely less than a fraction of one percent. And, unless they have personally done similar research and so can understand the data and potential pitfalls more clearly, even that enlightened fraction is highly likely to make some biased misinterpretation.
How can they not, when it is their own health they are investigating? Even a genius layperson examining the literature flawlessly would benefit from an interpretation provided by a neutral third party.
The comparison isn’t to the tools. Visual studio is the doctors blood analysis. The stack trace that visual studio spits out is the results of the blood analysis. Can anyone with some googling figure out what a stack trace means and what to do about it? MAYBE at best but realistically no. Now do you want to do the same with your heart? Brain?
You mention the average doctor but what about the average patient? How many people out there do you think will take the time to read through papers and citations and have the understanding to weigh options vs googling symptoms and going with the first result?
If you gave a common health problem chances are your doctor is more than capable of handling it.
If you have a difficult to diagnose problem that’s the time to take control over your health. You have to put in the time to trust but verify your own care.
Same thing with a difficult to debug code problem. It’s typically a function of time.
Right. This is why we don't allow consumers to access the Internet unless under the supervision of an IT professional never of the American Sysadmin Association guild. Lives are too important to be entrusted to the people who live them.
> Like, if I want an EKG, why can't I just walk in to a place and get it done at a reasonable price? And without a doctor's approval?
You're also paying for interpretation of your EKG at the same time. There are plenty of places happy to sell you home BP/HR/EKG monitoring kits, but you have to remember that you are paying for a doctor's time and clinical expertise when getting them in a hospital. It's not like a single EKG will tell you all that much about your heart anyway.
> As important as health is, and as much as Americans spend on it, it is shocking to me how gated everything is.
Agreed I had this issue as an uninsured university student with an Xray, and as one covered by my employer's insurance with an MRI.
In both cases I was stone walled to just get either, in the former I had to go to a clinic see an MD, come back get a physical and then get a referral for imaging off-site. And in the latter, I had to see 3 specialists, get a physical, have several weeks of Physical therapy and Xray imaging before the Insurance would cover it.
> Again, I pay for health insurance, but I still feel like if I want a quick EKG, it will take me 3 weeks to see a doctor, and by then I might be dead.
It was so exhausting just trying to make all the appointments and follow ups with a full work schedule that I haven't been able to get that MRI after all. I just assumed the worst and started to take matters into my own hands and started to do my PT exercises into my daily gym routine and will monitor the results myself.
> What am I missing? Are there legitimate safety reasons these mundane diagnostics are so locked down?
Its a protected Industry, the very supply of MDs is drastically capped in this country, its a controlled cartel.
MRIs are actually very expensive. Like they are just expensive... even in Europe. They’re costly to own and operate and maintain correctly.. just the labor alone. Unless you’re willing to pay out of pocket, I don’t see a problem with exhausting other options before jumping to MRI.
Also as for X-rays.. I think people freely getting Ionizing radiation isn’t exactly the brightest thing ever.
Also who pray tell, is going to read these studies?
Because they are too incompetent to be trusted to handle anything more complicated than shoes and canned food. As a former employee I could tell you stories.
> I would gladly even pay $50 per month for unlimited access to a place to just come in, get my blood sugar, kidney function, heart function, liver function, etc. tested once per month!
I've noticed my gym offers somewhat regular screening days which offer some (or all?) of that stuff, but it still costs extra. Reasonable (~$30?) but it would probably be something used more regularly if it was just part of the membership, and considered a normal thing. I don't even think they offer it monthly - I think it's quarterly.
After all, businesses exist to provide a service, and when I pay for that service if the owner gets to buy his wife shoes, that doesn't bother me.
What does bother me is that I can't walk into a clinic, let's call it "EasyLabs", and ask for an EKG right now, for $100, $200, $300.
It's the immediacy and tranparency of pricing, that's lacking and eliminating the doctor as middle man for tests and diagnostics that aren't harmful.
Money is not my concern.
The inefficiency is what is shocking to me.
To put the inefficiency of medical diagnostics in perspective, it is likely faster and easier for me to go out right now and buy a new $50,000 car, than it is for me to order my own MRI.
To me that just seems crazy.
But, as I said, maybe I'm missing something about the danger of getting tests like an EKG or an MRI needlessly.
For example, we know accumulated radiation from unnecessary x-rays would be harmful. So clearly not every medical diagnostic is safe to self-request.
Take a patient who has smokes about five cigarettes every day. Should we MRI their lungs to see if they have lung cancer?
The patient has the MRI, and doctors see some small spots in the lungs. Is this cancer? Or is it something that is completely harmless, such as scarring from childhood disease? To find out a needle biopsy is used. This is low risk, but it isn't no risk. The biopsy comes back clear. Does that mean that these spots are harmless, or does it mean that the person doing the biopsy missed them? At each stage we're perhaps causing fear and alarm and distress, and not really getting any useful information.
But we do know that this person smokes, and we do know that their health would be improved if we could help them stop smoking, and we know that nicotine replacement and support is an effective way to stop smoking for many people. It's probably a better way to spend the money.
Your example does not show that MRIs are harmful. It only shows that overreacting to the result of an MRI may be harmful. If you can just avoid overreacting then having more information can only help, never hurt. The results may seem useless now, but combined with other test results, advances in our medical knowledge, and tools like Machine Learning we may be able to draw useful inferences from that information later.
The discussion is about testing now, today. It's not about testing in 10 years time.
> can only help, never hurt
This is simply untrue. Assuming for a moment that people can avoid overreacting you're still ignoring the stress caused by getting a partial dx.
And if you're not going to do anything with the information it's pointless doing it: you've exposed people to risk (hospitals are low risk, not no risk, environments) for no purpose.
What you chose to do with your body is, of course, totally up to you. But you should stop spreading the FUD that imaging is harmless or that more information is always better.
> The discussion is about testing now, today. It's not about testing in 10 years time.
Indeed, and the results of tests done today may be relevant in ten years, even if we don't have the ability to draw useful information from them right now. If nothing else it may at least provide a baseline for comparison.
> Assuming for a moment that people can avoid overreacting you're still ignoring the stress caused by getting a partial dx.
Stressing out over an inconclusive test result would be overreaction. It's not as if stress is automatically a bad thing anyway, in moderation, or as if not knowing (or worse, being prevented from investigating) doesn't cause stress of its own.
> And if you're not going to do anything with the information it's pointless doing it...
I agree, so it's a good thing I never suggested that the results should be completely ignored. Just don't overreact.
> ...hospitals are low risk, not no risk, environments...
There is no such thing as a no-risk environment; moreover, imaging doesn't need to be performed at a hospital. A clinic is sufficient. Not doing the tests conveys its own share of risk; many conditions are much easier to treat when detected early, but you won't detect them early if you don't start looking until after symptoms manifest.
> ...FUD that imaging is harmless...
You have yet to provide any evidence that imaging is harmful, which hasn't stopped you from attempting to spread Fear, Uncertainty, and Doubt on the subject. The only FUD here is your own.
> and as much as Americans spend on it, it is shocking to me how gated everything is.
It didn’t always use to be this way. Then people started getting poisoned, sick and dying.
It’s not like the FDA existed when they ratified the constitution.
The opium epidemic proves the system is flawed and broken, it does not however prove that just throwing everything away will make things better.
>Are there legitimate safety reasons these mundane diagnostics are so locked down?
Healthcare is not my area of expertise either, but my understanding is that the short answer to your question is yes.
For a longer introduction to the issues surrounding letting anyone get whatever diagnostics they want to pay for, this Medlife Crisis video that came out today seems appropriate:
https://youtu.be/yNzQ_sLGIuA
Time on an MRI scanner (and to interpret and communicate the result) is a limited resource.
I fear unrestricted access would lead to over utilization by some people at the cost of less utilization by others. It could also lead to nontrivial psychological stress for people who can’t get a full understanding of the results. But I do think we need to strive for increased transparency from price lists to EHR interoperability to patient access to their own records.
MRIs depend on liquid helium, a scarce material by definition, but that's besides the point.
There is a high bar to becoming a physician because the consequences for error can be so incredibly high. I want there to be more physicians/access to medical care than ever but I don't think compromising on quality is the way to get there.
When it's cheaper to keep refilling an MRI scanner that boils off lots of helium, than buying one that loses only a little bit, then yes, you use a lot of helium.
It's not like we haven't discovered higher temperature superconductors that could be used, even if we didn't have helium.
EDIT: You can permanently fill 100 of these[1] per year with the boil off of one shitty MRI. Is uses about 1kg of He, so one year of world helium production would be enough to make one MRI machine for every 200 people. We are not constrained by helium.
This quote is from p61 but the whole thing is interesting)
> Note again the great difficulty large parts of the public, like the female veterans, have with translating small frequencies into percentages. Only 25% of the population could correctly convert 1 in 1,000 to 0.1%. Even among the highest education groups, at most 30% could solve this translation task. Lipkus, Samsa, andRimer (2001) even found that only 21% of well-educated adults could answer this question correctly.
You have prostate cancer. It's definitely cancer, this isn't a misdiagnosis.
Do you want the treatment, or do you want to do nothing?
This is a real choice faced by many men, in part because of the over-use of PSA testing.
It's a perfectly patronizing reason. If they're so concerned that test requires may be misinterpreted then the solution is better education. It is not their place to serve as gatekeepers.
There's a bunch of underinsured (or outright not insured) folk in the very locations where Walmart is opening these, so it has the potential to kill a couple of different birds with one stone. From a public benefits side, it gives a path of medical care for those that otherwise wouldn't have it (beyond say, an emergency room visit). It also lower prices by competing against insurance bloat.
In doing so, Walmart (may) be able to create a sustainable business by tapping a market (folk that aren't currently going for medical coverage anyway) that would otherwise be untapped.
This could also control costs if government managed systems (Medicare, Medicaid) partner with Walmart to provide payment. Easier to negotiate with Walmart as a single entity versus a network of vision and dental providers across the nation.
In Canada the govt doesn’t provide healthcare. It sets public rates for services, and then providers can provide those services to the public and get paid the set rates by the govt. This is called “single payer healthcare”.
You're right - for specialists and some GPs but not all. About half of the GPs are paid by their roster size, so-called "capitated payment". The idea being a doctors pay should be based on how healthy they keeps their patients rather than how many services they administer.
I only point that out for our American friends who might counter with "well isn't that a system ripe for abuse"
Really, do you have a source for that? I assumed everything, basically everything public insurance driven, which are most things, are negotiated by the government.
Just like how family/walk-in doctors get paid in 15 minutes increments so they try to rush as many patient through the day since they get paid for 15 whether it was a 2min appt or not. Which is why you see walk-ins packed full of people with well over an hour times, because not every meeting is fast.
On the other hand, I assumed the specialist got paid for their individual services they provide (and the orignal doctor got rewarded for the referral), since that's what they get referred to do, a specialized service which can be rated. It's also why radiologists ($800k/yt) are the highest paid doctor-type, complicated stuff requires good pay and they negotiate these on a case-by-case basis.
Edit: I found a paper talking about capitation in Canada and it mentions that Ontario is the only pr]ovince doing it and not all GDPs opted-into it. This sounds interesting - if a bit trusting of the people reviewing "performance". But I support testing out new payment systems, the current one could use some optimisation no doubt.
Same in Switzerland. Prices for services are fixed, and mandatory basic insurance won't pay more. Doctors and private hospitals are free to do their own thing, as long as their clients (or their additional insurance) are willing to pay the difference. I think only hospitals are in public hand, but they still have to go via the insurances for payment.
That’s certainly an option, but the meta-question is: which mechanism can produce health/pharma goods and services at lower costs and higher quality, markets or government allocation?
If the answer is the latter, then why aren’t we replicating that mechanism across other essential goods like food and clothing?
Some relevant questions are whether the demand is elastic and how difficult to compare and/or fungible the product is. Medical care is inelastic (without it you die) and difficult to compare (you don't get to try the same surgery with two different providers). Food is inelastic (even more so), and easy to compare, but many foods are very fungible (your supermarket will let you choose red white or yellow onions, but not which farm your onions come from). Demand for clothing is more elastic (you need it but you can probably wait for a sale), and it's easy to compare the items.
Medical care can be difficult to compare, but is that necessarily true across ALL medical care? There exists a high degree of fungibility in most preventive care: routine treatments like annual physicals, bloodwork, antibiotic prescription, flu shots, diagnostic imaging, etc.
The next question is: is there the same degree of fungibility for more major care, like tonsillectomies and appendectomies? Perhaps brain surgery and oncology is less fungible — but they are also perfect candidates for insurance coverage since they're catastrophic.
Same is true for food. I also wonder how affinity analysis can be applied to medical care. And - can the question of market vs government allocation be analyzed using "baskets"?
Most healthcare is not for life threatening illness. The bigger problem in healthcare in the US is that consumers almost never know how much a service will cost beforehand.
A "pure" competitive market would, but we don't have that and we're not going to get it. Eliminate insurance "networks", force hospitals to publish price lists and give the same price to every patient, make the medical statistics of every hospital and provider publicly accessible, and costs will plummet. As of now we have a hybrid system that combines the worst of both methods.
I think that's the key point. That would give insurances much more leverage to negotiate lower prices for everyone. Even other smaller insurances would profit... which would increase competition between the insurances... which would lower insurance costs for the people.
>then why aren’t we replicating that mechanism across other essential goods like food and clothing?
maybe because the competition doesn't work as well in healthcare sector? or that there isn't a whole scheme of inflated prices that insurance companies negotiate down to, but uninsured people are forced to pay?
If that's the case, then why are we seeing Wal-Mart attempting to compete in the healthcare sector with what seem to be competitive prices?
Doesn't seem to be limited to just Wal-Mart either. An Oklahoma City Hospital began posting its prices online and started a bidding war[1]. The hospital lobby seems to be overwhelmingly opposed to price transparency out of fear that it will lower prices[2], and there are Yelp-like directories that are beginning to provide price transparency allowing for competitive rates like $79 MRI's[3].
Walmart actually made a big difference in the health market years ago when they introduced the $4 prescription program, something like 300 pharmaceuticals that are available for $4. Even for people with health insurance this is lower than many insurance providers' co-pay pricing.
>If that's the case, then why are we seeing Wal-Mart attempting to compete in the healthcare sector with what seem to be competitive prices?
And it only took decades of skyrocketing healthcare costs (and probably margins) for walmart to enter the space. How many more decades (if ever) until prices drop down to level in line with other developed nations?
> And it only took decades of skyrocketing healthcare costs (and probably margins) for walmart to enter the space. How many more decades (if ever) until prices drop down to level in line with other developed nations?
Was this a natural consequence of the market, or are there other explanations for why such a delay came to pass?
Why is this question relevant? Let's say the reason was that walmart thinks their core competency is supply chain management, healthcare isn't part of that, and they only entered because the healthcare industry gravy train has reached insanely high levels that they simply could not refuse, what then? Should our response to this crisis be to wait until a megacorp comes by and saves the day?
This question is extremely relevant, because it can help us evaluate all policy options.
The current status quo in the US Healthcare system was not some crazy accident of the market, rather it was the inevitable result of a series of policies passed at state, local, and federal levels over the past half century.
The fact that health insurance isn’t portable, and is rather tied to employment is a consequence of the WW2 era wage ceilings imposed on private corporations, followed by the tax benefits enjoyed by employers that provide group insurance, followed then by the mandate on employers to provide health insurance. This is in contrast with other countries that employ private insurance, like the Netherlands and Switzerland, where insurance is tied to the individual, not the employer.
The lack of price transparency logically follows from the fact that patients never really care how much their treatments cost, since employer sponsored insurance covers everything anyway. Large corporations are less price sensitive than individuals, which exacerbates the price inflation over decades.
Certificate of need laws, where local hospitals get to decide if a new, competing hospital can open, and the residency system requiring 10+ years of schooling to practice resulted in inevitable supply constraints.
Medicare, which provides healthcare for free for the elderly, removed the most engaged buyers from the market, suffocating the price discovery mechanism. Not only that, the elderly tend to be the richest people in the country - those above the age of 55 account for 73% of wealth in America. Boomers are disproportionately rich, and yet they also enjoy some of the most generous welfare on top of that.
There are number of ways to approach solving this problem. One way is to add yet another band-aid on top of the system, burn down the system entirely, or identify the root causes and disentangle them from the system. This is the political question.
>The fact that health insurance isn’t portable [...]
Agreed.
>This is in contrast with other countries that employ private insurance, like the Netherlands and Switzerland, where insurance is tied to the individual, not the employer.
It's worth mentioning that in both countries, there's heavy government regulation. According to wikipeida, in the Netherlands 50% of premiums goes to some sort of government agency that redistributes money to private insurance companies depending on their claims, which makes it a quasi-public payer scheme. In Switzerland the premium is capped at a percentage of a person's income with the government making up the shortfall, and insurance companies can't make a profit.
>The lack of price transparency logically follows from the fact that patients never really care how much their treatments cost, since employer sponsored insurance covers everything anyway.
Doesn't this argument apply to insurance schemes in general, both public and private?
>Large corporations are less price sensitive than individuals, which exacerbates the price inflation over decades.
I'm skeptical about this claim. Sure, they have more money sloshing about than individuals, but insurance premiums across the entire workforce adds up.
>Certificate of need laws, where local hospitals get to decide if a new, competing hospital can open, and the residency system requiring 10+ years of schooling to practice resulted in inevitable supply constraints.
Agree, although I'm weary of assigning significant blame due to this factor. Are doctors making record wages? Are hospitals making record profits?
>Medicare, which provides healthcare for free for the elderly, removed the most engaged buyers from the market. Not only that, the elderly tend to be the richest people in the country - those above the age of 55 account for 73% of wealth in America. Boomers are rich, and they also enjoy some of the most generous welfare on top of that.
I'm skeptical how big of an effect this can be. Wikipedia has a chart that shows medicare spending as percent of GDP[1]. If you combine that with total US healthcare spending by GDP[2], you see that it accounts for less than a fifth of total US healthcare spending.
> It's worth mentioning that in both countries, there's heavy government regulation
No disagreements that there exists regulation that can be helpful. Definitely an important part of the discussion. Even in Singapore, which is largely a market based system driven by price discovery relies on a healthy (heh) amount of regulation. In the US, the food system is largely market-based, but the FDA (as well as state and local health departments) impose important regulations.
> In Switzerland the premium is capped at a percentage of a person's income with the government making up the shortfall, and insurance companies can't make a profit.
Keep in mind that in the US, health insurance companies report an average profit of ~5%. Even if you eliminated that entirely, you wouldn't see any savings worth writing home about. I work at an insurance company, and the majority of claims I see are pretty asinine. $500 added to provide sign language service to a deaf patient, or $300 charged for a papoose used while giving a child a cleaning. Because of the third-party-payer model in which the care is priced and paid for AFTER the services are rendered, the patient has little skin in the game. In the best case (for the patient) the insurance company simply pays the asking price (resulting in a sort of moral hazard), and in the worst case, the insurance company doesn't cover it and the patient gets a surprise bill in the mail.
> Doesn't this argument apply to insurance schemes in general, both public and private?
Yes, it's another reason why using insurance to pay for all care can be a sub-optimal way to allocate resources. Not having skin in the game can result in patient overconsumption.
> Agree, although I'm weary of assigning significant blame due to this factor. Are doctors making record wages? Are hospitals making record profits?
Yes, and yes[1][2]
> I'm skeptical how big of an effect this can be. Wikipedia has a chart that shows medicare spending as percent of GDP[1]. If you combine that with total US healthcare spending by GDP[2], you see that it accounts for less than a fifth of total US healthcare spending.
The effect I'm talking about is removing the largest consumers of healthcare (rich old people) from the market, which impacts how the ultimate price of goods/services is determined by the market.
Clothing is a wildly different market. Imagine if the only way to get clothes were through a bespoke tailor, in person. No other way. And you often had—had—to get a very specific kind of jacket or whatever, no option to sub some other article, or else you or your kid dies or lives in pain or something. That’s healthcare. If clothes worked that way that market would suck, too.
Explain France and Switzerland then. Both use market mechanisms for delivering outpatient care. Or are these not European nations with universal healthcare?
Limiting the question to price and quality but ignoring availability might (I don’t know) favor markets and definitely ignores an (arguably) basic obligation of government but not markets.
I’d argue that the basic obligation of the government is welfare, at its core. Everything else is an implementation detail in service of that.
If the (regulated) market can bring down equilibrium prices to the minimum, then the government’s role could be to provide health stamps or cash to those in need, similar to food stamps (which can arguably be reformed).
I think that’s a fair expectation of government. It may be that the market can deliver care at the lowest cost but what if the market delivers that lower cost by limiting supply? Say they don’t offer service in some areas or limit some procedures?
Then the next question is: historically, which systems of resource allocation have been able to successfully avoid supply shortages of the thing in question, markets or government allocation?
Market prices are currently set based on 1-3x multipliers of Medicare reimbursement, so by definition the government already handles health care at lower costs.
Commodifying health care has proven to be disastrous in the US because it's, in practice, impossible to "shop around" — not even including cases where the "customer" is unconscious or in a life-threatening situation where "shopping" would be ridiculous, the profit models of health care centers are forcing many to close, leaving people with few choices in their immediate area, exacerbated by the "network" coverage model of insurance companies where you may not even be able to go to certain hospitals or doctor's offices.
Interestingly, though, improvements in supply chain management are making it possible to centrally-plan commodities like clothing. Multinational companies like Wal-Mart and Amazon are doing this already, in fact.
> Market prices are currently set based on 1-3x multipliers of Medicare reimbursement, so by definition the government already handles health care at lower costs.
I work in insurance, and I can tell you right now that $25 for a cleaning (per this article) is significantly lower than the amount for a cleaning (procedure code D1110) set by Medicare/Medicaid. You can look it up yourself by visiting the FAIR Health code lookup tool (https://www.fairhealthconsumer.org/dental/results), and setting the ZIP code to that of Carlton, GA (location of the Wal-Mart clinic), 30627. The average allowed amount is $64.
> Commodifying health care has proven to be disastrous in the US because it's, in practice, impossible to "shop around" — not even including cases where the "customer" is unconscious or in a life-threatening situation where "shopping" would be ridiculous, the profit models of health care centers are forcing many to close, leaving people with few choices in their immediate area, exacerbated by the "network" coverage model of insurance companies where you may not even be able to go to certain hospitals or doctor's offices.
Ignoring emergency health services (which is the minority of health spending), I'm not sure that we have enough information to irrefutably prove that preventable and planned care cannot be successfully commodified. A common theory around why we haven't been able to commodify healthcare in the US is due to a lack of price transparency, and the fact that employer sponsored health insurance removes the price sensitivity from buyers[1][2].
> Interestingly, though, improvements in supply chain management are making it possible to centrally-plan commodities like clothing. Multinational companies like Wal-Mart and Amazon are doing this already, in fact.
They aren't centrally planned, though — they are subject to market competition (see: DHL, UPS, FedEx, FlexPort, Maersk, etc). Their ability to be major "central planners" by controlling large parts of the supply chain is predicated on their ability to fend off market competition, and the moment they fail to do that, this manifests as a market opportunity for new competitors to take their place, wherever in the supply chain the large corporations fall short.
> If the answer is the latter, then why aren’t we replicating that mechanism across other essential goods like food and clothing?
We do/have. Water, electricity, phone services (and other communication), roads, child care and and whatever else the romans have done for us have all had successful government implementations. Food and clothing typically haven't been included in this list because choice is more important for them and the market does a good job at providing them, but even there I think there's room for a government foodbank/clothes bank style option.
> Water, electricity, phone services (and other communication), roads
These are all natural monopolies due to the limitations of public infrastructure. Such natural monopolies don't necessarily exist for goods/services like food, clothing, and medicine (most notably, over-the-counter generic medicine). Communication is largely left to the market, rather than government coordination/pricing.
> but even there I think there's room for a government foodbank/clothes bank style option.
Either that, or just providing the poor with money to buy food at market-rates, i.e. food stamps.
Notably, food and to some extent clothing (textiles) have been very much the concern of the state, or of the way the state’s organized. What’s changed is that both got way the hell cheaper to make and we settled on some good, more-or-less stable regulations and systems of management to keep things from getting too nutty too fast.
Government doesn't provide service directly almost anywhere else in the developed world. Especially the services Walmart is targeting (optometry, dental cleaning, etc).
Universal coverage doesn't mean government employs every provider directly.
Hm. Wife had eye check at big box store. The guy said "Oh, you have Macular Degeneration. Nothing to do about it sorry. Just go home and go blind".
She came home in tears of course. So I said "Go to a reputable ophthalmologist and get a real opinion". So she did.
Of course nothing is wrong with her eyes (despite the power-of-suggestion effects she experienced, but miraculously cleared up once she got a reliable exam). The Dr did say "I can see how they made the mistake; you have some small adhesions to your retina, but they'll clear up by themselves"
So no, I'm not going to a big box store to get my medical care. Never mind the price. I'll get a professional, or go without. Can't be worse than our experience at the discount-home-goods place.
Your experience (or rather, your wife's experience) seems to be about the difference between seeing an optometrist and an ophthalmologist.
I don't know if the optometrist she saw was unusually incompetent or if any optometrist would have done the same, but in any case, everyone she dealt with was a "professional" (even if, maybe, different professions. These big box retailers are not - and can not - hire people without qualifications to provide these services.
I think you may be drawing an unsound conclusion here.
For what it's worth...those eye glasses places are run by optometrists (usually) and not an ophthalmologist. An ophthalmologist has more medical training.
They are all independent of the store and just pay rent. But they are all professionals...
Edit: Also if you have a real medical issue w/ your eye, definitely see an ophthalmologist. Optometrists are for glasses and minor eye issues...they aren't going to be doing surgery on you.
When you get your eyes checked for glasses you go to an optometrist. Doesn't matter if it's big box store or a local guy--they have the same credentials.
An ophthalmologist is an MD who specializes in eyes, and that's who you want to go to when you have a more serious problem. 2 completely different things, and not really anything to do with where the optometrist was located.
It sounds like a very incompetent optometrist (and if they weren't one, someone basically impersonating one). They're eye specialists after all who go to a 4-year post-undergraduate program, just not M.D. doctors. At a minimum, they should presumably have told your wife to book an appointment with an ophthalmologist immediately.
Yes, but the big box store likely has a fresh grad for the same reason that the local Jiffy Lube has the new tech and Swift has the new driver and Applebees has the new chef.
These high margin low volume chains hire the bare minimum of professional (in their industry) and it's where the bare minimum goes to gain experience and put a few years of work on their resume so they can become something better and get a better job. These entry level employers tend to be slave drivers so once people have the experience under their belt to get a better job they generally do.
If you have a routine thing that needs to be done then these places work great because you're not paying for unnecessarily skilled labor. If you have something odd a more skilled professional is usually advisable.
It's pretty common for opthamologists to fill gaps in their schedule with general optometry type visits, and sell corrective eyewear for profitability reasons. The exams are quick and straightforward, and the margins on frames, lenses and contacts are pretty decent.
Yes an ophthalmologist can do that, but it's not their primary function. The vast majority of times you go get a lens prescription, you're going to an optometrist.
My wife and I both often have trouble hearing, especially in noisy environments. My hearing level is those environments is much worse than anyone else around. At a bar, I effectively can't understand what anyone is saying unless they're shouting right next to me. With no noise, I have amazing hearing.
I went to Costco with my Wife and we both got our ears checked because they offered free hearing checks. Both of us were told we hear amazing, and were subjected to jokes about our marriage.
We concluded that their only goal was to sell hearing products, and if they couldn't fix the problem, they didn't diagnose it.
I suspect your wife's experience at the "big box store" was the same: Not anything they could fix, so they just sent her away.
Yeah well I'd pay for the medical care I need, regardless of insurance. Not everybody can do that, and I know it. Kid of a 'first-world' problem I guess.
But get used to a brave new world of stand in line/shotgun medicine where you get a diagnosis from the hip of a bored assembly-line 'doctor' who long ago forgot why they went to medical school.
I'm just waiting for these massive corporations to get into the automation of Pharmacy work. I know a number of highly paid (110k+) pharmacists who largely:
A) count pills
B) put pills into orders
C) do retail
D) answer questions/customer service
Meanwhile, the industry is being flooded with new graduates from dozens of schools...If this isn't a case for automation of A-C, I don't know what IS a case for automation in healthcare.
You've got it backwards. Pharmacists are hired because it's legally required. They're there to catch the dosage mistakes, look out for potential interactions, and to answer questions about medication and the proper usage. You cannot legally distribute prescription medication without a pharmacist physically present.
CVS and Walgreens would love to get rid of the pharmacists -- they hate that each store needs a couple $110k/year pharmacists just to handle the legal requirements and to be on-site for the few cases where something needs extra attention. That's why they put them to work doing the manual retail side of it to get the most for their dollar.
It's legally required because even with a prescription, an untrained person can't just walk to a hypothetical drug store with everything on the shelf and safely select what's written down. There are too many chances to make mistakes, misreading the label, self diagnoses and prescription of dangerous substances, etc. This can be addressed by automated, human-free system with tech we have today. Your doc sends a valid Rx, a box dispenses your drug. I don't know if it would be cost effective today, but we could do it and it stands to reason that one day it will be cheaper than doing it (validating substances and dose) with one highly trained human counting pills by hand at every single location.
Potentially dangerous drug interactions and instructions can be solved by automation for what can be automated and tele-pharmacists in all others.
This can be addressed by automated, human-free system with tech we have today. Your doc sends a valid Rx, a box dispenses your drug.
Sure, what would be necessary is a GUI that was as usable and flexible as the doctor's hand-written scribble while being standard enough across the country that any doctor could use and every single drug could be dispensed by it.
Which is to say that this is a really massive undertaking and opposition from a multitude of angles, including opposition from companies that have invested in most half-assed solution. Which is to say, this likely won't happen or it will require more than one more corporation dipping their toe in this.
A very large part of what pharmacists do is double-check the doctor's work. Mistakes, miscommunication, overlooked drug interactions, etc. In a sense the purpose of a pharmacist is having an accredited person dispense the medication as part of the pharmacy's liability insurance.
Because it's not the case that the pharmacist is automatable. A small fraction of the work is completely un-automatable and the easily automatable stuff is just busy work. Even if you automated it they'd still have to hire a pharmacist, he would just have less to do.
Drug interactions are not a lookup. Some people have problems some do not. We don't even have interaction data on all possible combinations of two different drugs, much less all the 6+ different drugs that some people are taking. There is a lot of "Educated guesswork".
For someone only taking one drug for a couple weeks and the a year latter a different drug for a few weeks it is easy.
Seems like there would be the possibility of WFH pharmacists whose job is to do the educated guesswork on any newly observed combo. Log it into the system after some validation and voila we have timeless knowledge for all who come later, automated at low costs.
I saw this (or one like this) in action in China at a hospital. There were 15+ windows to line up for the pharmacy and each one had a lot of 10+ people. I was in shock because in the US even 2 people in like would take forever.
The procedure is, you scan your ID at a machine attached to a pillar. The screen tells you which line to line up in. When you get to the front of the line you hand your card to the nurse the medicine comes down a chute.
The line moved fast. I received my medicine in a matter of minutes. Also I paid for the medicine w/ the doctor that prescribed it - so none of this BS about "oh your insurance doesn't cover this, you haven't met your copay" talk that half the pharmacists seems to spend their time with. The doctor told me what to do with it and fielded any questions.
Moving prescriptions or getting a new prescription especially for controlled substances or things that require prior authorization from insurance co is just a PITA from a user perspective.
Exactly, the pharmacist is there to provide expert advice when you have a complicated prescription or combination of prescriptions. You can tell by these comments that the HN crowd leans young -- not enough people dealing with chronic illnesses who have seen the value in having a consult with the pharmacist when you pick up your medication.
My wife has a handful of chronic illnesses and I want her to be able to ask questions of someone who has been educated in the role, method of action, correct dosages, and possible interactions of her medications.
In my experience, medication interactions are both solidly in the wheelhouse of physicians and taken quite seriously. As someone below pointed out, it's still a huge problem, and having more eyes and a distinct training/set of skills in the pipeline is a win for everyone.
I do not know this as a fact, but I don't believe US pharmacists are able to adjust dosing on the fly - though of course they can and do reach back out to physicians with questions.
I had an experience recently that really solidified my respect and appreciation for pharmacists though. I was standing in line behind a older gentleman who had maybe a 10 minute conversation with the pharmacist. I tried to mind my own business but couldn't help but hear the overall gist. He was very confused about what his medication was for and especially how to take it. The pharmacist clearly had a relationship with him and wrote down schedule based on the meds he was already taking. He thanked her by name and she told him she's give him a call later in the week to check in on how he was managing.
I was curious (and the last person in line) so I asked her about her work and how often she ends up so involved. Apparently she made lots of calls throughout the week to people, and people came in confused about their medications often enough. By percentage it sounded like a minority of the patients, but her assistance was obviously super important to a lot of people in the neighborhood.
I don't think I've ever asked a pharmacist for more info on my life, but I'm very grateful they exist as a resource. At the very least, I think it's important we don't think of pharmacies as counting factories that can be replaced by robots. And while I'm all for dropping the price of healthcare across the board, I hope the kind of value that kind of one-on-one interaction at least gets it's fair shake in any accounting done thinking about making a switch to tele-pharmacies and the like.
You realize there are reasons we have old people and computer tech support memes right? Replacing humans in the loop would do absolutely nothing to help.
From what I've been told, physicians spend a relatively short amount of time actually studying the details of drugs while pharmacists spend several years and know considerably more about dosing, interactions, etc.
Doctors do not do a great job of balancing the behaviors of and interactions between prescriptions. You could say that they should do a better job--probably justifiably--but pharmacists do that for a living.
My doc, who's a great diagnostic, has a fantastic network and usually knows his shit prescribed a pain killer (Vimovo, which in addition to the pain killing compound contains a proton-pump inhibitor. The compound which reduces acid production in the stomach, so that the pain killer is much more gentle to it).
He advised to take it after food, which is true for any old pain killer (for example Ibuprofen), but not for such specific medications.
In fact it should be taken half an hour before a meal.
That's the reason why it's prescription only and deployed by a pharmacist, who immideately caught it an gave me correct advice.
Physicians (and other prescribers such as dentists) don't even necessarily know what all medications a patient is taking. In theory they can check through the regional Health Information Exchange or Surescripts but in practice things fall through the cracks. This is a leading cause of preventable medical errors.
The unfortunate part of modern American medicine is that the pharmacy isn't likely to know all the medications the patient is on either. I'm currently going through a minor situation but have discovered that health insurance has, in some cases, switched to a model of partnering with specialized pharmacies for certain treatments. You're forced to use a specialized pharmacy for one specific condition while your day to day corner chain is completely excluded.
You can even get that without having some prescription that your insurance has made a special deal with. I currently have 3 prescriptions at Walmart and 1 at Safeway, all of them generics that I'm not using insurance for. I'm paying the cash price for the Walmart ones, and using GoodRx for the Safeway one.
It used to be all 4 at Walmart, and then something utterly ridiculous happened. For the non-US readers who won't believe this idiocy, I swear it is true. We really do put up with this nonsense.
One of them was for irbesartan. I'm supposed to take it twice a day, 150 mg each time. The prescription was written for 30 x 300 mg tablets, which I split in two (irbesartan comes in a rod shaped tablet that you can easily split it two by hand).
This is $9 cash at Walmart.
But then there were some irbesartan recalls (although not affecting the manufacturer of any tablets I had). There was a shortage of 300 mg tablets, and Walmart was having trouble refilling my prescription.
So we had my doctor change it to from 30 x 300 mg tablets to 60 x 150 mg tablets. The cash price for 30 x 150 mg is $9 at Walmart, same as 30 x 300 mg. (I'd guess that for this drug, most of the cost is in filler and binder, so that is probably not unreasonable). So I'd expect 60 x 150 mg to be $18.
Walmart filled that, and when I went to pick it up...it was something like $300. WTF!? So they double checked, and found out that it had actually been written as 180 x 150 mg. They redid it as 60 x 150 mg, which dropped the price to about $100. So, still a big WTF.
According to GoodRx it should be $24 cash (still a WTF...why not $18?). Since this is one that GoodRx thinks has a good cash price at Walmart, GoodRx does not offer a coupon for it there. I showed the pharmacist the listing in the GoodRx app, and he agreed to honor that price, so I got my prescription for $24.
GoodRx did have a coupon for Safeway, for 60 x 150 mg for around $13, so when it was time to re-fill that, I move it there. (That changed to about $18 next month).
I ran out of re-fills about 3 months later and so needed a new prescription, and by then 300 mg was readily available again so asked for 90 x 300 mg, which was $21 with a GoodRx coupon at Safeway.
I mean this may be partially true for a retail pharmacy setting, but is much different in a clinical one.
Even in an place like Walgreens where customer service is a big part of the job, the idea that it's all a pharmacist does feels simplistic and reductionist and plainly wrong. There's lots of coordination with the patient's doctor and insurance and other pharmacies they might use.
It's like saying programmers just type into a keyboard.
That's one thing I've wondered about as well. Most of what pharmacists do can be automated and should be automated. That doesn't mean pharmacists should be without work. Their expertise should be applied elsewhere. What's the point of getting so much education to simply count pills?
Better yet, why can't your doctor just send the request to a pharmacist facility and have them fill the order and deliver it to your home? Why does he hand you a piece of paper that you have to bring to a pharmacist? When you give blood, you don't take the vials/tubes to the testing facility. The doctor's office sends it where it needs to go.
Most of A, B, and C are done by techs. Pharmacists are there to manage the techs. But predominantly they are there to be prevent or be held liable for mistakes and loses/thefts of very high value inventory.
The automation of pharmacy needs to happen in two areas:
1. Count pills and package them.
2. Drug interaction detection.
1 can be automated. In fact the warehouse style pharmacy can do all that. The doctors (or you) send the prescription to the pharmacy warehouse. They ship the medicine to you.
2 can also be automated. Drug interaction are sets of rules and the detection can very well be done with machines.
Pharmacists are Health Care professionals and they're part of the chain of credibility. You absolutely want credible people dosing out medicine, double-checking, etc..
In no uncertain terms should unqualified people be answering questions about anything healthcare-related.
Just the smallest questions I ask my pharmacist, I can tell she is super well trained: relatively clear when she can be, when she doesn't know she indicates this, for things out of her bounds she refers to the doctor. Very careful communication.
For a little over $100K + all the training, I'd say it's a reasonable deal. That's about the professionalism you'd want before having someone chime in on your health.
Maybe it could be reformed but I think pharmacists are valuable.
Pharmacy revenues will remain constant. The only difference is that instead of paying pharmacists, all that money is just going to sit in the caymans, with all the other automation gains.
Should we bring back telephone operators too? The price for phone service (especially long distance) has dropped since phones were invented, surely some of that is due to automation and tech advances.
Do you think technical progress is making life worse for the average person? I realize it's popular opinion (and I tend to agree) that it's disproportionately benefiting the richest. But that doesn't mean most people aren't benefiting from the cost/time savings that new technology has brought. Curious to hear why you think that way.
I have serious doubts that tech is making us happier, overall, and that is’s actually significantly improving productivity, outside a few areas where is has done so massively such that the effect is still strongly positive.
Exceptions for certain areas like medical research, obviously, but really, things were fine before Netflix and free long distance and such.
I'm just talking about pharmacists and telephone operators. I dont mind pharmacists and I didnt mind telephone operators. My life isnt much better now that telephone operators are gone.
It is absolutely not a do nothing job. Every one I've ever interacted with seemed overstressed from the insane work load/hours, if anything. 12-14 hour shifts are common.
It's an okay gig on average, currently. Chains keep buying the smaller guys out, reducing hours and support staff, increasing demands of metrics, and offering lower and lower pay to new grads. It doesn't help that new schools keep opening and applicant numbers do not increase in quality or quantity. The BLS anticipates 0% job growth in the next 10 years.
This is great. Walmart has a reputation to protect so at the very least I can trust what they say.
I've had a hard time getting a dentist I can trust. The business reminds me of car mechanics that are always looking to sell you additional services. And as a layperson, it's hard to know when you are being sold services you don't need. They love people with insurance since they can get them to buy without much pushing.
> This is great. Walmart has a reputation to protect so at the very least I can trust what they say.
I've had a hard time getting a dentist I can trust.
Do you think that dentists don't also have a reputation to protect? What makes you take polar opposite views of the two?
I get what they're saying. Walmart is literally known by every single person in the country (and outside the country as well). It's much less effective to bitch about getting ripped off by the local DDS and have people see about it and also care about it. If a bunch of people went online and were talking about getting ripped off by Walmart, it could very easily get picked up by the media if the claims were legit and then could affect the stock price.
I think people are also much more likely to talk to one another about the "shitty new Walmart healthcare service" because they know everyone knows Walmart and might use it. It's far less likely that you warn people about one single DDS office in your town unless perhaps that specific service provider came up in conversation.
It's not the same. I think it's a matter of scale. Walmart, because of its size, will often have more checks and balances. They will not take a chance to mar their reputation. Walmart wants to keep people's trust. It's worth billions to the company. It's not 100% but I feel more comfortable if I'm not constantly being pushed additional services to buy.
Most dentists I've dealt with run their practice as a small business. Usually, it's a few dentists. They need to constantly sell. I understand that they need to stay in business but it's so constant that you never know where you stand.
I'm not saying that all dentists are like that it's just hard to find one that you can trust. Just like car mechanics.
How does your scale argument apply to companies like Amazon which gleefully sell counterfeits and trash on their site, or allow scammers to run rampant?
What makes you think that Walmart is different here?
Local dentists have a reputation to maintain, but the impact of reputational damage is generally limited. If they end up with 10 Yelp reviews complaining about fillings not lasting as long as they should or being overcharged, it may negatively impact the volume of patients they have or prices they can get away with charging.
Walmart, on the other hand, actively has a target on its back. And with $524bn in revenue last year and almost $33bn in EBITDA[1], it's one of the most deep pocketed targets around. Any minor issue has the potential to spin itself into a national news story, and malpractice lawyers would be giddy to nab a patient they can use to take a stab at Walmart's pursestrings. And just think of the stars in their eyes if they stumble upon enough complaints to get certified as a class action and be able to really dig into the clinical guidelines and operating procedures for deficiencies to exploit.
Not to say the service they offer is likely to be world class. But between their existing institutional competencies in operations[2] and the potential liability concerns, it is likely to garner a reputation for being consistently and predictably acceptable[3].
[2] Walmart's operational standards are notoriously demanding and exacting across their supply chain network. They could easily bring that to bear in running their clinics and enforcing compliance with clinical guidelines and SOPs from their medical providers.
[3] Walmart's reputation for mediocre product quality isn't an accident, it's a deliberate choice. And one that takes a considerable amount of effort to enforce and consistently maintain across the board for decades. They use their scale to get an incredibly detailed view of consumer behavior (because what people say rarely matches what people do). Then turn around and squeeze their suppliers to get a bill of material that minimizes return rates and maximizes consumer satisfaction within the constraints of price points determined by prior consumer behavior.
Not totally agreeing with op, but I can understand a few differences: you don't complain the same way with a doctor and with a company. people tend to just switch. a brand like Walmart may be subject to a global scrutiny and raise the level globally.
Does Walmart have such a great reputation? They sell a lot of cheap crap. (I should know; I shop there all the time. b^)
Unless your employer is paying for every bit of it, dental insurance is a scam. They almost never pay enough in any given year to catch up with the premiums. You're better off taking out loans for dental procedures you can't immediately afford. And, as you imply, one is more likely to choose wisely when one is footing the bill oneself.
Dental insurance can be a scam, it also can be worth it depending on what the premium is. Some time ago I was offered insurance through work that covered two teeth cleanings in a year for slightly less than the cost of paying for the cleanings out of pocket. Since I always get my teeth cleaned twice a year I was happy to take that insurance. Nowadays my employer provides me with dental without premiums.
Other than those two times I didn't find buying dental insurance worth it and paid out of pocket.
Given the quality I've seen in American megastores (I've seen bicycles seem really dangerous to ride -- is there no institution that regulates vehicles?), my knee-jerk reaction is that this is a terrible idea.
At the same time, I'm all for accessible and good healthcare, so let's see how this plays out.
Wal-Mart sells something like 2 million bicycles a year. If they're actually selling "really dangerous" bicycles then it should be easy for you to point at some actual statistics about it. After all, in America there are regularly recalls for things like
"we manufactured 600 bicycle forks that might crack and pose an fall hazard"[1]
"we made 800 bicycles where the caliper might come into contact with a broken spoke"[2]
"we manufactured 4,100 steer tubes that can become loose"[3]
I didn't say that Walmart sells dangerous bicycles. I said that some supermarkets sell bicycles that seem dangerous to ride, so I'm wondering if the regulations are strict enough. More specifically, when I was in the USA I've seen bicycles at the K-mart, so I was referring to those. It seems I'm not the only one who think those bikes are terrible:
Still, you make a good point in showing that there actually are at least some regulations. Whether they are strict enough and focus on the right points is not entirely clear to me.
Even if it's middle of the road service performed by inexperienced people starting out their careers and looked down on by professionals with more experience (i.e. basically how Walmart tire center is viewed in the automotive world) it still provides an alternative keeping the prices of higher class options in check.
As a Walmart tire tech, I'd like to recommend everyone that not every tire shop is equal, even within Walmart. Our next door Walmart acc generates a lot of horror stories that we get to fix. Also some local non-Walmart tire shops do even worse. Like forgetting to tighten lug nuts. Heard that one several times about a local (and quite respected!) tire shop.
If I can walk in without an appointment, see a doctor after a reasonable wait, and then get a prescription for antibiotics that can be filled on the spot, then I’m 100% on board with this.
I live in the Ohio Valley area and the biggest problem we run into is seasonal allergies. That doesn't sound so bad as its just a stuffy nose at first, however after a couple of weeks it turns into a nasty sinus infection. Getting an antibiotic through a traditional Dr. can take many days (or even weeks). Going to the "after-care" is inconvenient and can take hours.
If I could pop into WalMart when I feel this coming on, I would do it in a heartbeat! Especially if it meant that I didn't have to do all the insurance stuff. Even better if the whole visit costs the same as my insurance co-pay ($30)!
I'm pretty sure there's been a few times in the last few years that my wife has called up a doctor on the phone and gotten a prescription for her sinus infection, and then just went to Target and filled it. She didn't have to physically see a doctor. I'm also pretty sure it was a service that her health care provided, so you should ask your health care provider if they have something similar.
At a prior large tech company, one of the coolest benefits compared to my current small startup was Teladoc[0]. I have no idea what the actual cost is or anything, but it was pretty much this.
This! When I was in China the experience was as described by your parent comment except the doctor insisted she give me a prescription for herbal medicine since it's better for me... (Had the flu, REALLY wanted nyquil, but it's illegal there it seems).
This is hilarious. I'm no universal healthcare idealist, but there is something to be said about health services having the wrong incentives in doing it for-profit. What incentives do for-profit pharmaceuticals have to keep people healthy? Potentially none. What incentives do they have to keep people sick? Probably billions of dollars if not more.
The problem is you can't risk your health. When buying a product you can risk a "clever" company that sells you a subpar product, but you can't really risk a "clever" pharmaceutical that sells you a subpar medicine or service.
> What incentives do for-profit pharmaceuticals have to keep people healthy?
In a competitive market when people aren't happy with a product or service they take their business elsewhere. Over time companies with bad intentions get weeded out or never get off the ground.
The problem is you shouldn't be making that decision when you are already sick and you discover your insurance won't cover. Additionally the current healthcare market is not what I would call competitive. Only a handful of insurance companies have some kind of monopoly, not to mention how it's tied to having a job. All of this assumes that getting sick is a choice like driving a car.
Yes, it absolutely does. The vast majority of 'healthcare' is operationally mundane, and not hyper-specialized such as those who are in car accidents might require.
Most public systems are quite inefficient, and without any possible market pressures (Canada healthcare act makes it technically illegal to sell healthcare services that are provided by the gov.) then those inefficiencies sink in.
Because there's a weird inelastic demand for certain services, pure market-oriented solutions won't work for 'car crashes' but they definitely could for most other things.
Walmart taking on healthcare is a very meaningful event, they could feasibly operationalize the more mundane issues to the point wherein it's the cheapest in the world for such services. This is hugely positive news.
I'm curious why the reasons you elucidated aren't enough to make you a universal healthcare idealist. Do you mean by this that you don't want universal care or that you don't care about the issue or something else? If you mean by this that you don't want universal healthcare under what circumstances would you want this?
I ask not to engage in a debate or to try to change your mind. I won't respond to anything you write. I'm just curious about people who don't advocate for universal healthcare what their reasoning is.
For the record, I think everyone should have access to the healthcare system and that no one should profit by denying a person care. I also don't think that being rich ought to grant you better access or quicker access to the system since resources are limited and the type of care or quickness or care should not be influenced by money.
I think it's a logistics problem. Perhaps every state could offer a free healthcare option. Private healthcare is available in single-payer countries but you still pay taxes, and in the U.S. health insurance companies have changed the system so that they are always in control and there isn't any real competition for any other insurance. For prices to go down there should be real competition for these services, but I don't see that anywhere. Either government fully controls and taxes, or private companies control the government and in turn the market.
> What incentives do for-profit pharmaceuticals have to keep people healthy?
Having better outcomes than the other for-profit pharma down the street, thus more customers, thus more money. Of course, if there is no competition at all then the incentives change, but this is not (yet?) the case.
I have been thinking for years that the only economic entity that might be able to take this on is Wallmart.
I believed that if there was a single thing Barack Obama could do, it would have been to convince Wallmart to heavily invest in healthcare, the point of building clinics.
Walmart is quite a different beast than other companies. Walmart, by strategy, does not compete on margin, they compete on volume. Since high margins are a problem for volume, they actively try to suck out margins in a product all along the value chain.
Walmart pushes suppliers to improve their own cost metrics and has enough power to do it. They basically use their leverage to force down prices, knowing they'll make it up in the long run on volume.
This is a very, very different approach to business than basically anywhere else, and possibly has ever existed and it's one of the few magic things that makes Walmart what it is.
The 'literati' classes love to hate on Walmart, but consider how powerful this machine is: it basically sucks profits and inefficiency out of the value chain like a vacuum, handing over the surpluses to consumers. They basically enable 100 million Americans to live at a standard of living not otherwise possible.
Health Care is the most bloated sector in the entire world, and there's so much juicy fat to be cut, if there's any operational entity has the scale, operational ability, customer reach, efficiency to pull this off it's walmart.
I hope they expand into basic medicine, family medicine, all of the basic kind of testing, and insurance.
I can't say I'm otherwise a huge fan of Walmart, but if they end up raping and pillaging healthcare in the US, they could literally be creating the biggest benefit capitalism ever provided for Americans.
I'm a huge, huge fan of this. I haven't stepped into a Walmart in years, but I'm thinking I need my teeth cleaned ...
I'm a graduate student in a small city. I would gladly use this dental cleaning service. I haven't been to the dentist in like 2 years because I really can't afford it. I actually get my prescriptions via Walmart already without insurance because it cheaper than using the insurance given to the grad students.
I heard a podcast on this recently where they cynically concluded that Walmart is doing this primarily to have more control over the healthcare costs of its employees. Will a Walmart doctor recommend AN expensive MRI for a Walmart employee if his boss doesn't like that?
Ideally it would be a solid hedge against the government going nowhere with improving the cost of healthcare. If it makes people get checked up more often, it could reduce overall healthcare costs because more issues get caught early.
Combine it with an app that offers specific recommendations and reminders based on your health profile, and you'd have an interesting startup. (this probably won't happen due to HIPAA/privacy issues and not being in Walmart's general wheelhouse).
Walmart using their market power in one industry to charge below market rates in another, driving out competition. This is going to destroy health care options in areas that are already under served.
When called to Congress to testify about it 15 years from now, Walmart execs will exclaim "It's about competition: if we hadn't done it, Amazon would have!"
? The people providing healthcare today, are as you described, except they have huge, fat, ridiculous margins. They commit what would be point blank fraud in any other country, all day, every day.
Walmart is a massive machine that operates by design on thin margins. They force out surpluses all the way down the value chain and in their own operations and instead of selling at max margin, they sell at low margin, because they know they win in the long run.
Walmart might be exactly what you'd invent if you wanted to provide healthcare at the best price to the most people. There's the possibility they could be more efficient than any system anywhere as most public systems are full of fat as well ... certainly more than the 5% or so margin Walmart might take in.
a megacorp that stiffs employees on health care gets into health care. Cool story, Walmart, hope the Walton children enjoy their slice of that $3.5 trillion pie.
This is great news. Every six months I go to the dentist for a checkup and teeth cleaning, and it's always the same: they look at my teeth for a few minutes with the mirror thing, scrape off some plaque with the pointy thing, polish my teeth with the spinning thing, then I do the flouride rinse and leave. It usually takes less than half an hour, and then they bill my insurance $275 for it. It's ridiculous, and there's no way this requires a graduate medical degree, it could be done by someone who took a three-week mail-in training course. Keep dentists' offices with DDS's around for major surgeries or unusual situations, but for routine checkups this is fine.
> it could be done by someone who took a three-week mail-in training course.
Sounds like you have healthy teeth, but your comment is fairly ignorant of the fact that nearly everything you described isn't done by someone with a graduate medical degree, but generally is done by a dental assistant/hygienist . I wouldn't want someone to touch my teeth if they haven't practiced using the instruments in a classroom. This isn't a programming course..
> Dental assistants receive their formal education through academic programs at community colleges, vocational schools, technical institutes, universities or dental schools. Graduates of these programs usually receive certificates. Although the majority of academic dental assisting programs take nine to eleven months to complete, some schools offer accelerated training, part-time education programs or training via distance education. [0]
Took my step daughter to the dentist this morning. An x-ray and impressions. Whole process took 14 minutes. And that includes having her pose for front face and side face photos. Not a dentist in sight, just an assistant.
Dental insurance, especially, is a scam. The amount of "benefit" you get really is pretty low if $bad_things happen - a few thousand at most.
It's more like a pre-payment plan that lots of people don't pick up the item the care they pre-paid for.
I was going to go without because I saw what my insurance had been paying out. I figured I'd save a bit and I could "self-insure" in case of bigger problems. Joke was on me - I got billed about 6x as much as the insurance company. So now I pay for dental insurance because it gets me access to the "real" prices, not because I really want "insurance".
That sounds bizarre. Lots of people with medical insurance don't have dental insurance. I do and it covers cleanings but, as I recall, a cleaning is around $100 or so. (I get 3 cleanings a year and at different times the insurance I've had sometimes covered the third and sometimes didn't.)
Crowns are around $1200 which I end up covering half of.
In my experience, dental is actually relatively free market. Some providers (like mine) charge a bit more than insurance covers for things like fillings and I just pay it. But, even if you don't have insurance, rates are pretty reasonable for 30-60 minutes of a professional's time. My accountant certainly isn't any cheaper.
The dentist was overpriced, but cleanings were free to new but delta was paying $750 hence Monopoly money. Then they charged me $350 for fixing a cavity but refunded me $140 after their accountant told them to. So yes Monopoly money. I’d hate to get cancer even though my insurance is relatively good with at $1050 out of pocket max.
I used to work for a company that did claims benefits management.
For all their (many) faults, insurance companies are often very interested in hearing about provider fraud.
Oftentimes, there may be no direct action from _your_ report, but it might help establish a pattern, versus "oops, we mis-coded the procedure/who provided it".
I'm pretty sure that my insurance company has a standard rate that they will pay out for procedures. And I'm also pretty sure they wouldn't pay for a $750 cleaning.
needed a root canal a few years back. went to the first local place. got an estimate of $2500. way too much for my blood. called around, got someone else to do it for around $1300. Found out there's actually a guy closer who does most for around $900+. But... I went with the $1300 lady. She was fine, and have been going back since. It's a bit of a drive, but the initial price was enough of a 'trust' factor for me, and I trust now that if/when I need something done, I need it done, and that her price will be reasonable. It might be a bad assumption on my part, but I did have that initial savings years ago. She'd be having to jack up everything else quite a lot to be trying to gouge me, and I don't think it's happening. She's just in a less expensive part of town, generally sees less affluent patients, and everything is priced for that market. That it's a 20 mile drive to get there doesn't bother me.
I can tell you from experience that an improperly done root canal can come back to bite you years later. Had one done by IHS[1] when I was in 6th grade. During my 1st year in college I woke up with mouth pain that was really, really bad. Had to get a parent to come get me and drive me to a dentist. He took x-rays and found out I had an infection growing since the initial root canal[2]. He prescribed antibiotics and a massive pain reliever (Percodan[3]). It took four weeks for the infection to go down enough for surgery. The doctor said it might come back because they might not get it all. It took two more operations (5 and 10 years later) to fix it all.
1) given what's happened to so many other people, I feel I got off cheap.
2) no, the IHS dentists did not see this growing and it was probably slowed by the multiple antibiotic prescriptions for step throat in high school.
3) Took it for two weeks, I'm still amazed I was functional enough to take tests and program. That stuff is a whole lot of don't care in one bottle.
understood. the procedure referenced above was from... gosh now, 9 years ago. no issues with it (I've had other teeth issues but not her fault). Wife had a bad root canal done by a 'fancier' place which went bad a few years later.
In theory the dentist is supposed to glance over your mouth and screen for gum cancer or other issues. So a three-week mail course is certainly an exaggeration.
The dentist office has to roll up all their costs under the services they provide. So the $275 contributes to all the staff wages and benefits, office space, etc. That is why for example the HVAC repairman charges $300 for changing a $5 capacitor in your AC. Places like Costco/Walmart can reduce the costs by keeping a steady stream of customers and sharing building space, etc.
That's extremely unusual, I've been a patient at probably 20 different dental practices and I've never had a dentist do the cleaning, only the dental hygienist.
>there's no way this requires a graduate medical degree
The actual cleaning itself is done by a dental hygienist, which requires an associate's degree. The dentist only shows up and the end to see if he/she sees any problems.
This is in Bloomberg. Who themselves have announced they are Mike's propaganda. Skimmed the article and couldn't find any reason it's a story /today/. Why is it a story today? Speculate.
The US healthcare system is third world standard. Great if you're rich, horrendous if you're not. Just like say, India, for example. US is the richest country on earth. Any story about US healthcare not mentioning how much worse it is than every other industrialized nation runs the risk of impersonating propaganda.
So if this isn't propaganda they've disguised it effectively.
Remember when we used to make jokes about Pravda. Radio Moscow. Here we are in the free world. We can do better about sensible policy discussion than this. Really.
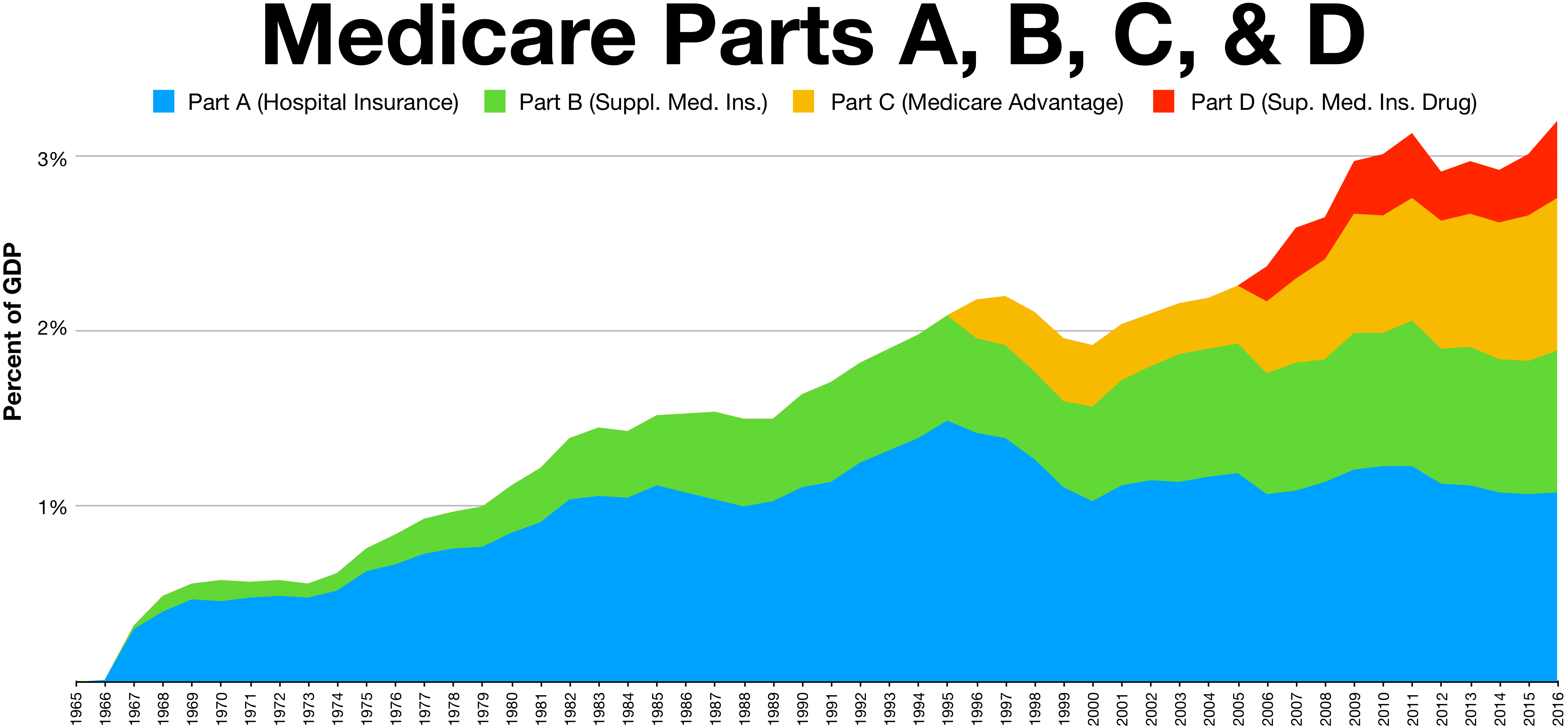{kind=link}
It is astounding to me how locked down certain medical tests are.
Like, if I want an EKG, why can't I just walk in to a place and get it done at a reasonable price? And without a doctor's approval?
And I pay for insurance. But I just want to be able to monitor my vitals myself, whenever I feel like it.
It seems like it would drive higher utilization of equipment and lower prices if these types of diagnostic tests were readily available at a place like a CVS or a Walmart.
I would gladly even pay $50 per month for unlimited access to a place to just come in, get my blood sugar, kidney function, heart function, liver function, etc. tested once per month!
As important as health is, and as much as Americans spend on it, it is shocking to me how gated everything is.
It hurts my health and my pocketbook simultaneously!
I've always wondered why a company like Walmart doesn't just provide $20 EKGs, and $25 tooth cleanings.
Like, why is so easy to get a hamburger at any time of day, but like pulling teeth to just run somewhere and get a quick, inexpensive EKG to make sure everything is ok with your heart..?
What am I missing? Are there legitimate safety reasons these mundane diagnostics are so locked down?
Or are these services available and I just don't know about it?
Again, I pay for health insurance, but I still feel like if I want a quick EKG, it will take me 3 weeks to see a doctor, and by then I might be dead. I don't want to see a doctor, I just want an EKG done for my own peace of mind.
But health Care is not my area of expertise. So perhaps there are very legitimate reasons these diagnostics and labs are so difficult to self-request at reasonable prices.